

Abstract
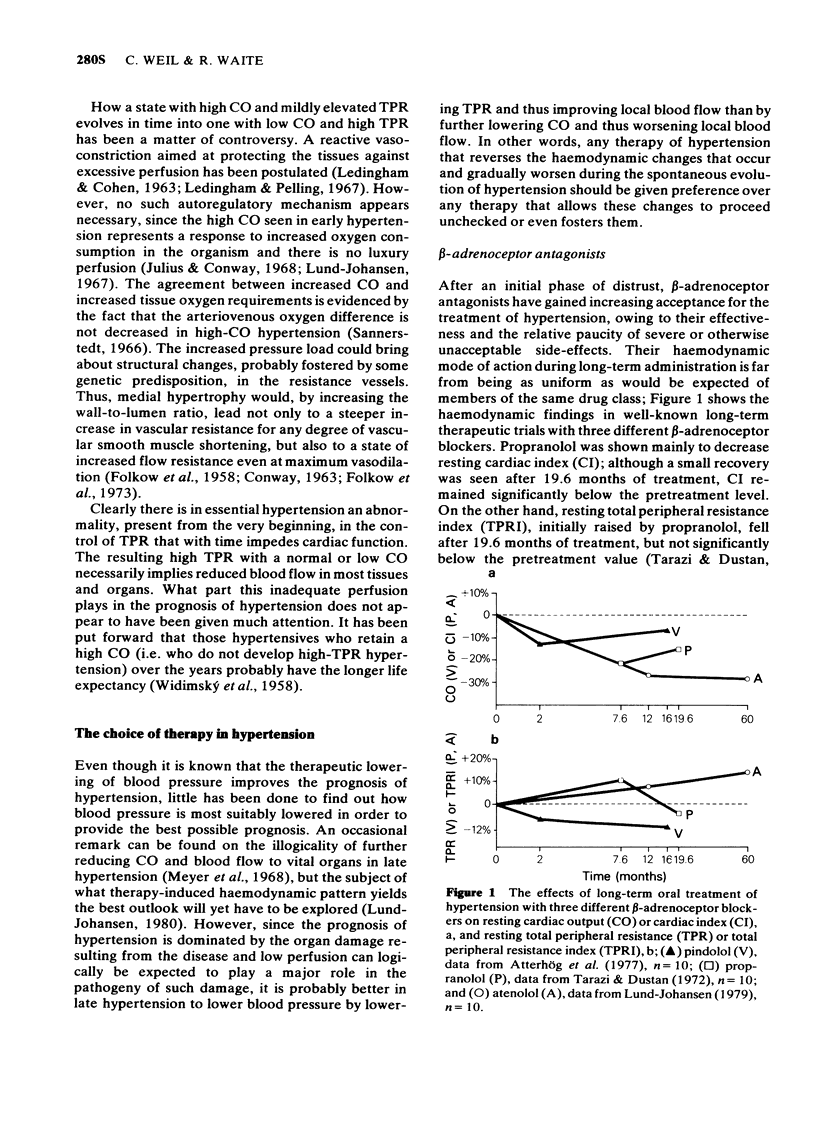
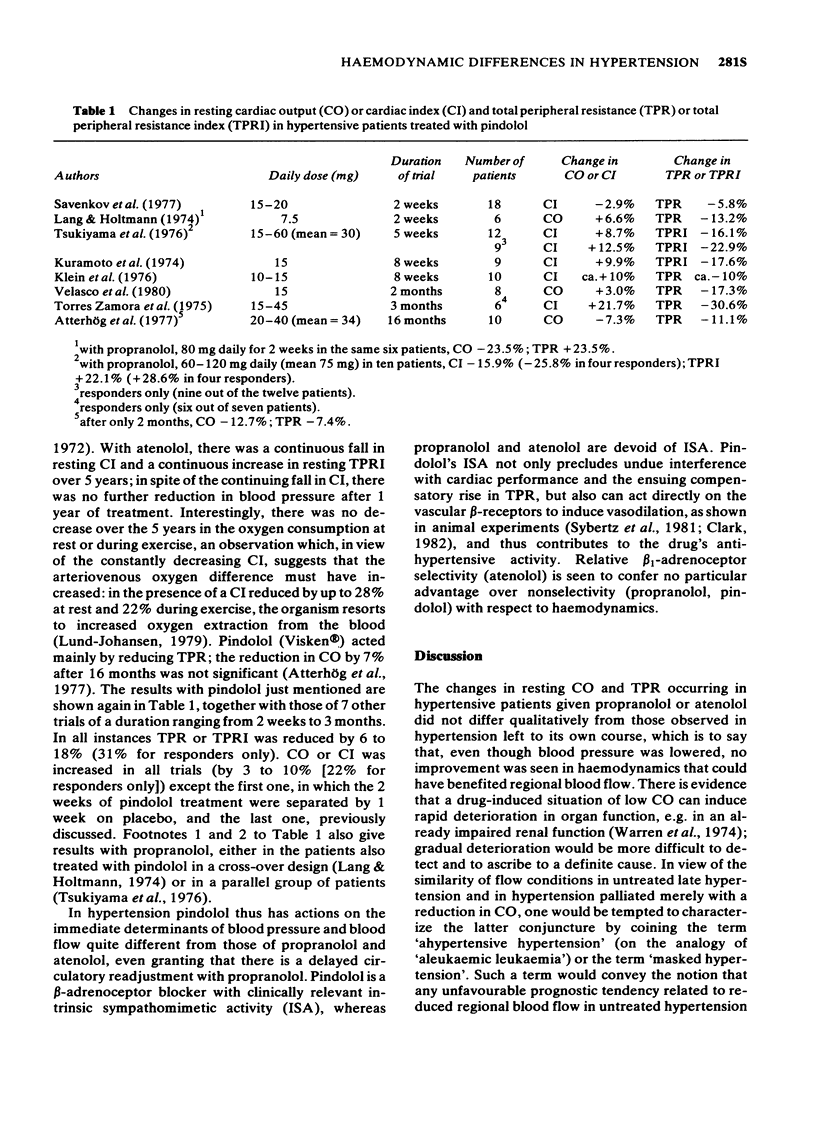
1 As a rule, hypertension progresses from an early stage with a high cardiac output (CO) and an inappropriately normal total peripheral resistance (TPR) to later stages with a normal or decreased CO and a high TPR. 2 Low CO and high TPR can be considered detrimental to the blood perfusion in the tissues and organs and thus to their functional and structural integrity. 3 Among beta-adrenoceptor antagonists, some lower blood pressure by reducing CO, thus bringing about a reactive increase in TPR. The result is that, even though blood pressure is reduced, the haemodynamic conditions commanding regional blood flow are qualitatively similar to those in untreated hypertension. To what extent these circumstances may curtail the benefit expected from blood-pressure reduction deserves careful investigation. 4 Pindolol, a beta-adrenoceptor antagonist with an appropriate degree of intrinsic sympathomimetic activity (ISA), lowers blood pressure while lowering TPR and not unduly reducing cardiac performance. These features should on theoretical grounds lead to a greater improvement in the prognosis of hypertension.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Atterhög J. H., Dunér H., Pernow B. Hemodynamic effect of long--term treatment with pindolol in essential hypertension with special reference to the resistance and capacitance vessels of the forearm. Acta Med Scand. 1977;202(6):517–521. doi: 10.1111/j.0954-6820.1977.tb16874.x. [DOI] [PubMed] [Google Scholar]
- CONWAY J. A vascular abnormality in hypertension. A study of blood flow in the forearm. Circulation. 1963 Apr;27(4 Pt 1):520–529. doi: 10.1161/01.cir.27.4.520. [DOI] [PubMed] [Google Scholar]
- EICH R. H., PETERS R. J., CUDDY R. P., SMULYANH, LYONS R. H. The hemodynamics in labile hypertension. Am Heart J. 1962 Feb;63:188–195. doi: 10.1016/0002-8703(62)90195-3. [DOI] [PubMed] [Google Scholar]
- Eich R. H., Cuddy R. P., Smulyan H., Lyons R. H. Hemodynamics in labile hypertension. A follow-up study. Circulation. 1966 Aug;34(2):299–307. doi: 10.1161/01.cir.34.2.299. [DOI] [PubMed] [Google Scholar]
- FOLKOW B., GRIMBY G., THULESIUS O. Adaptive structural changes of the vascular walls in hypertension and their relation to the control of the peripheral resistance. Acta Physiol Scand. 1958 Dec 15;44(3-4):255–272. doi: 10.1111/j.1748-1716.1958.tb01626.x. [DOI] [PubMed] [Google Scholar]
- Frohlich E. D., Kozul V. J., Tarazi R. C., Dustan H. P. Physiological comparison of labile and essential hypertension. Circ Res. 1970 Jul;27(1 Suppl 1):55–69. [PubMed] [Google Scholar]
- Julius S., Conway J. Hemodynamic studies in patients with borderline blood pressure elevation. Circulation. 1968 Aug;38(2):282–288. doi: 10.1161/01.cir.38.2.282. [DOI] [PubMed] [Google Scholar]
- Klein W. W., Brandt D., Fluch N., Goebel R., Holzer H., Pöch G. Hämodynamische Langzeiteffekte eines Beta-Rezeptorenblockers (Pindolol) bei primärer arterieller Hypertonie. Adv Clin Pharmacol. 1976;11:79–85. [PubMed] [Google Scholar]
- LEDINGHAM J. M., COHEN R. D. THE ROLE OF THE HEART IN THE PATHOGENESIS OF RENAL HYPERTENSION. Lancet. 1963 Nov 9;2(7315):979–981. doi: 10.1016/s0140-6736(63)90677-9. [DOI] [PubMed] [Google Scholar]
- Ledingham J. M., Pelling D. Cardiac output and peripheral resistance in experimental renal hypertension. Circ Res. 1967 Jul;21(1 Suppl):187+–187+. [PubMed] [Google Scholar]
- Lund-Johansen P. Haemodynamic long-term effects of atenolol at rest and during exercise in essential hypertension. Postgrad Med J. 1977;53 (Suppl 3):99–101. [PubMed] [Google Scholar]
- Lund-Johansen P. Haemodynamics in essential hypertension. Clin Sci (Lond) 1980 Dec;59 (Suppl 6):343s–354s. doi: 10.1042/cs059343s. [DOI] [PubMed] [Google Scholar]
- Lund-Johansen P. Hemodynamic alterations in hypertension--spontaneous changes and effects of drug therapy. A review. Acta Med Scand Suppl. 1977;603:1–14. doi: 10.1111/j.0954-6820.1977.tb19353.x. [DOI] [PubMed] [Google Scholar]
- Lund-Johansen P. Hemodynamic consequences of long-term beta-blocker therapy: a 5-year follow-up study of atenolol. J Cardiovasc Pharmacol. 1979 Sep-Oct;1(5):487–495. doi: 10.1097/00005344-197909000-00001. [DOI] [PubMed] [Google Scholar]
- Sannerstedt R. Hemodynamic response to exercise in patients with arterial hypertension. Acta Med Scand Suppl. 1966;458:1–83. [PubMed] [Google Scholar]
- Savenkov P. M., Doshitsin V. L., Grudtsyn G. V. Primenenie beta-adrenergicheskogo blokatora viskena (prindolola) u bol'nykh arterial'noi gipertoniei. Kardiologiia. 1977 Oct;17(10):62–66. [PubMed] [Google Scholar]
- Tarazi R. C., Dustan H. P. Beta adrenergic blockade in hypertension. Practical and theoretical implications of long-term hemodynamic variations. Am J Cardiol. 1972 May;29(5):633–640. doi: 10.1016/0002-9149(72)90164-6. [DOI] [PubMed] [Google Scholar]
- WIDIMSKY J., FEJFAROVA H. M., FEJFAR Z., DEJDAR R., EXNEROVA M., PIRK F. Der jugendliche Hochdruck. Arch Kreislaufforsch. 1958 Apr;28(2):100–124. [PubMed] [Google Scholar]
- Warren D. J., Swainson C. P., Wright N. Deterioration in renal function after beta-blockade in patients with chronic renal failure and hypertension. Br Med J. 1974 Apr 27;2(5912):193–194. doi: 10.1136/bmj.2.5912.193. [DOI] [PMC free article] [PubMed] [Google Scholar]