

Abstract
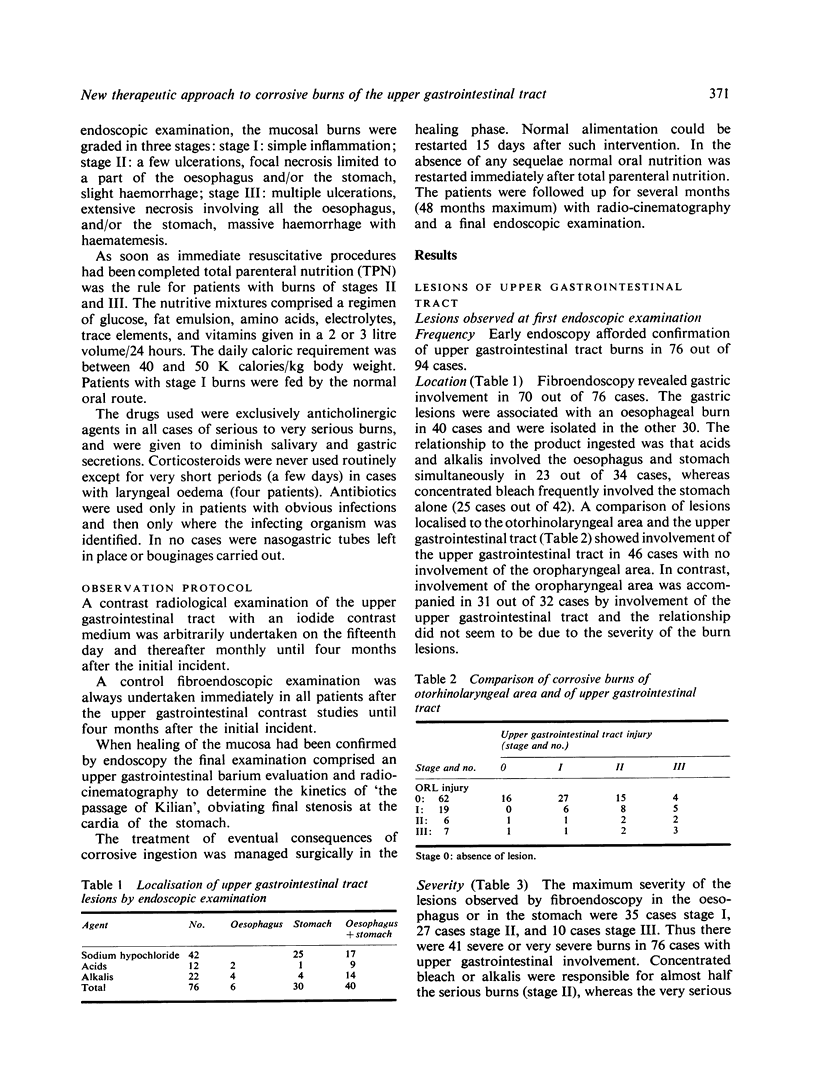
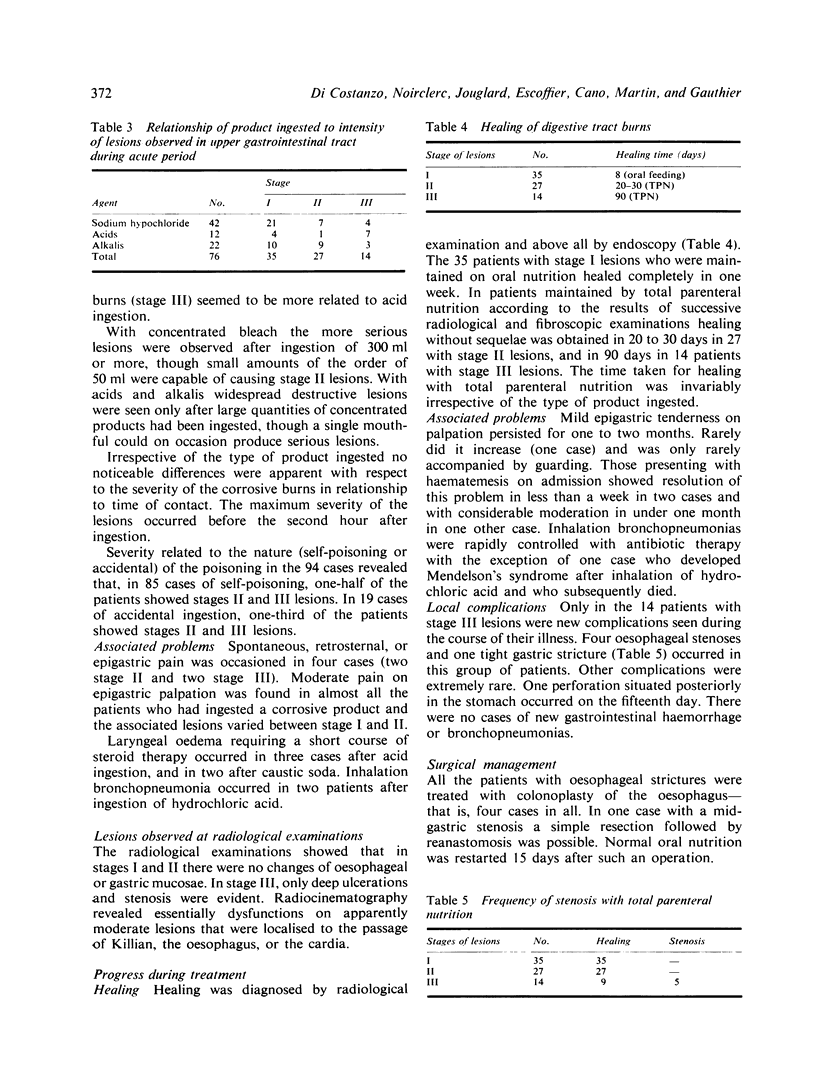
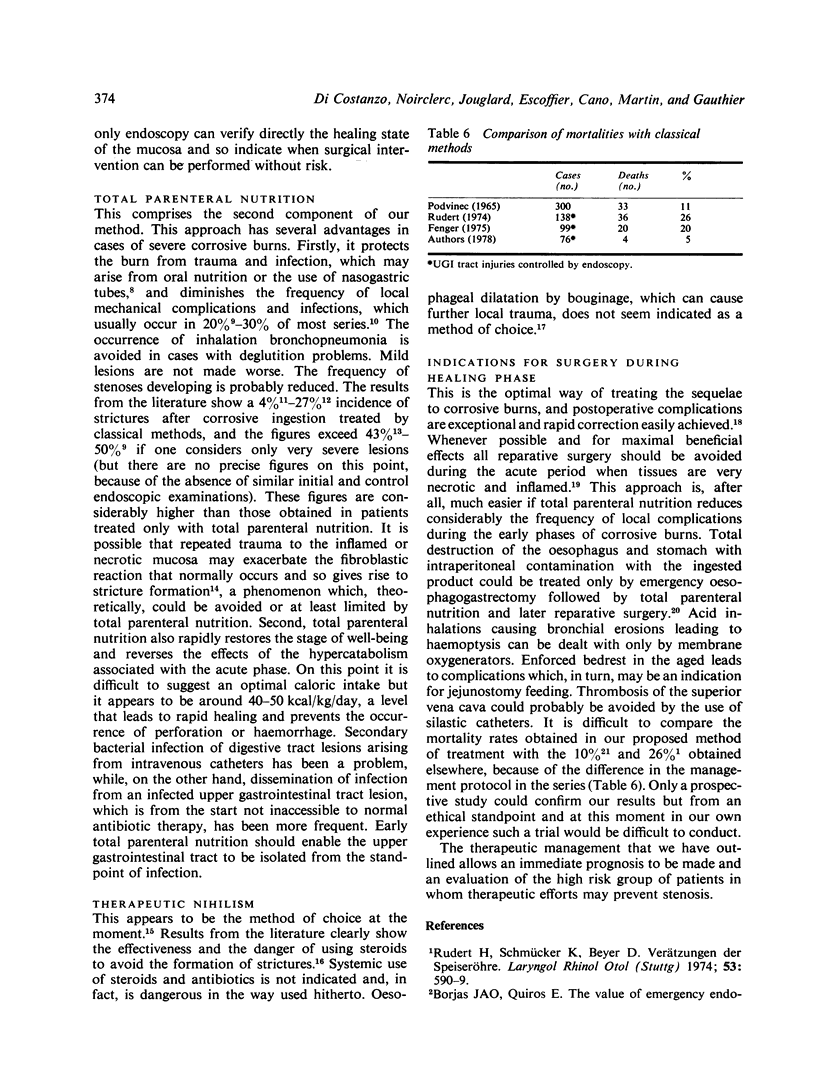
The therapeutic approach to the management of corrosive burns of the upper gastrointestinal tract leaves a considerable morbidity and a heavy mortality rate. This work evaluates the effectiveness of a new therapeutic approach given to 94 consecutive patients. The management has been based on three major points: (1) the definition of extent of upper gastrointestinal lesions by immediate fibroendoscopy; (2) immediate protection of the upper gastrointestinal tract by total parenteral nutrition in cases with serious burns (41 cases), normal oral nutrition being allowed for minor burns (35 cases); (3) reparative surgical procedures for any of the sequelae of such burns during the fibrosing phase. The results were as follows: (a) healing, depending upon the degree of burn, occurred between eight to 90 days; (b) the frequency of subsequent local complications was small with total parenteral nutrition started a few hours after ingestion of the corrosive product; (c) after reconstructive surgery no serious complications occurred; (d) the overall morbidity stayed at a very low level (four patients). We conclude that the general prognosis of a severe burn of the upper gastrointestinal tract, without other trauma, is appreciably improved by the very early institution of total parenteral nutrition.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Balasegaram M. Early management of corrosive burns of the oesophagus. Br J Surg. 1975 Jun;62(6):444–447. doi: 10.1002/bjs.1800620606. [DOI] [PubMed] [Google Scholar]
- Bleicher B. Brulares par ingestion de caustiques. Etude statistique. (A propos de 50 observations. JFORL J Fr Otorhinolaryngol Audiophonol Chir Maxillofac. 1973 Dec;22(10):861–864. [PubMed] [Google Scholar]
- Chung R. S., DenBesten L. Fiberoptic endoscopy in treatment of corrosive injury of the stomach. Arch Surg. 1975 Jun;110(6):725–728. doi: 10.1001/archsurg.1975.01360120043008. [DOI] [PubMed] [Google Scholar]
- Dubost C., Celerier M., Leclerc J. P., Kaswin R., Choquart P. Les grandes brûlures caustiques oeso-gastriques de l'adulte. J Chir (Paris) 1976 Dec;112(6):385–408. [PubMed] [Google Scholar]
- Imre J., Kopp M. Arguments against long-term conservative treatment of oesophageal strictures due to corrosive burns. Thorax. 1972 Sep;27(5):594–598. doi: 10.1136/thx.27.5.594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knox W. G., Scott J. R., Zintel H. A., Guthrie R., McCabe R. E. Bouginage and steroids used singly or in combination in experimental corrosive esophagitis. Ann Surg. 1967 Dec;166(6):930–941. doi: 10.1097/00000658-196712000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ortega Borjas J. A., Quiros E. The value of emergency endoscopy in caustic esophagogastritis. Am J Gastroenterol. 1973 Jul;60(1):70–73. [PubMed] [Google Scholar]
- PODVINEC S., BOGICEVIC J., SAVIC D., JOKANOVIC D. CAUSES PR'ECOCES ET TARDIVES DE LA MORT APR'ES L'ESIONS CORROSIVES DE L'OESOPHAGE. Ann Otolaryngol Chir Cervicofac. 1965 Mar;82:115–126. [PubMed] [Google Scholar]
- Ray J. F., 3rd, Myers W. O., Lawton B. R., Lee F. Y., Wenzel F. J., Sautter R. D. The natural history of liquid lye ingestion. Rationale for aggressive surgical approach. Arch Surg. 1974 Sep;109(3):436–439. doi: 10.1001/archsurg.1974.01360030088023. [DOI] [PubMed] [Google Scholar]
- Reyes H. M., Hill J. L. Modification of the experimental stent technique for esophageal burns. J Surg Res. 1976 Feb;20(2):65–70. doi: 10.1016/0022-4804(76)90100-1. [DOI] [PubMed] [Google Scholar]
- Ritter F. N., Gago O., Kirsh M. M., Komorn R. N., Orvald T. O. The rationale of emergency esophagogastrectomy in the treatment of liquid caustic burns of the esophagus and stomach. Ann Otol Rhinol Laryngol. 1971 Aug;80(4):513–520. doi: 10.1177/000348947108000413. [DOI] [PubMed] [Google Scholar]
- Rudert H., Schmücker K., Beyer D. Verätzungen der Speiseröhre (Bericht über die Verläufe von 138 Fällen sowie eine Nachuntersuchung von 46 Fällen) Laryngol Rhinol Otol (Stuttg) 1974 Aug;53(8):590–599. [PubMed] [Google Scholar]
- Savic D., Pejakovic S., Mihaljevic B. La localisation des lésions des voies digestives d'après l'agent corrosif. Ann Otolaryngol Chir Cervicofac. 1970 Oct-Nov;87(10):680–681. [PubMed] [Google Scholar]
- Taillens J. P. La cortisone dans les oesophagites corrosives aiguës. Pathogénie d'action et effet thérapeutique. Ann Otolaryngol Chir Cervicofac. 1970 Oct-Nov;87(10):621–636. [PubMed] [Google Scholar]
- YARINGTON C. T., Jr, BALES G. A., FRAZER J. P. A STUDY OF THE MANAGEMENT OF CAUSTIC ESOPHAGEAL TRAUMA. Ann Otol Rhinol Laryngol. 1964 Dec;73:1130–1135. doi: 10.1177/000348946407300424. [DOI] [PubMed] [Google Scholar]