

Abstract
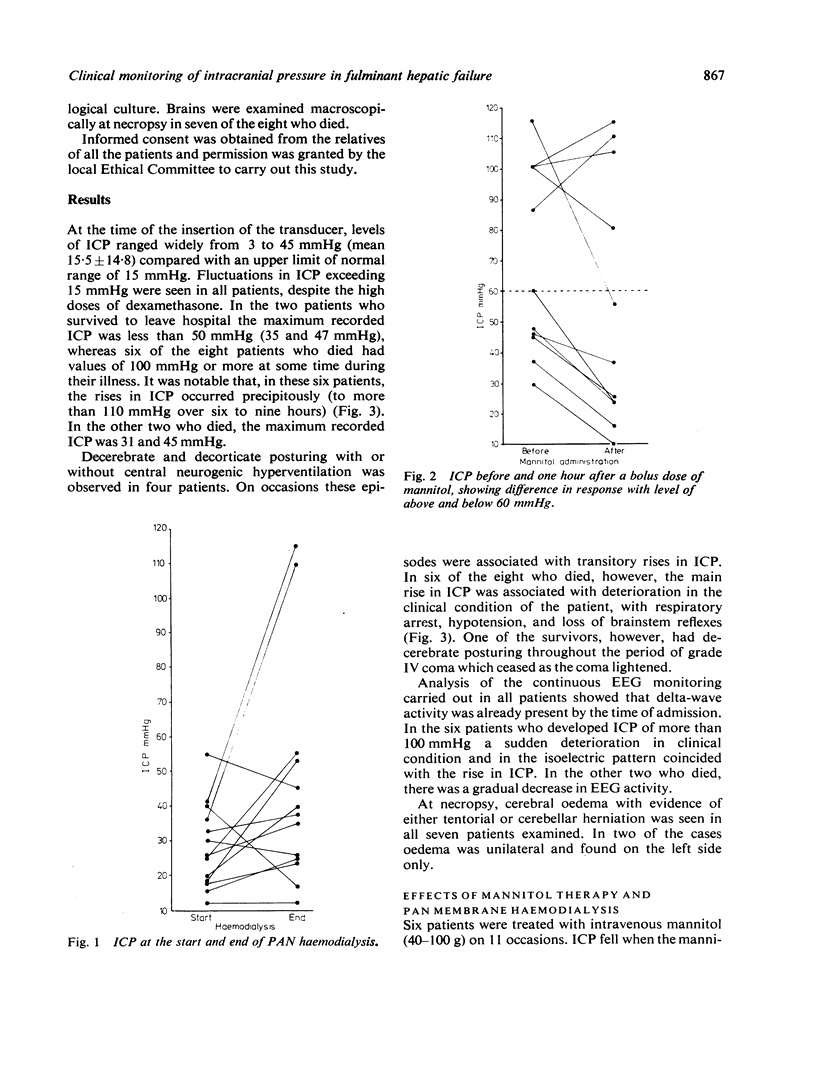
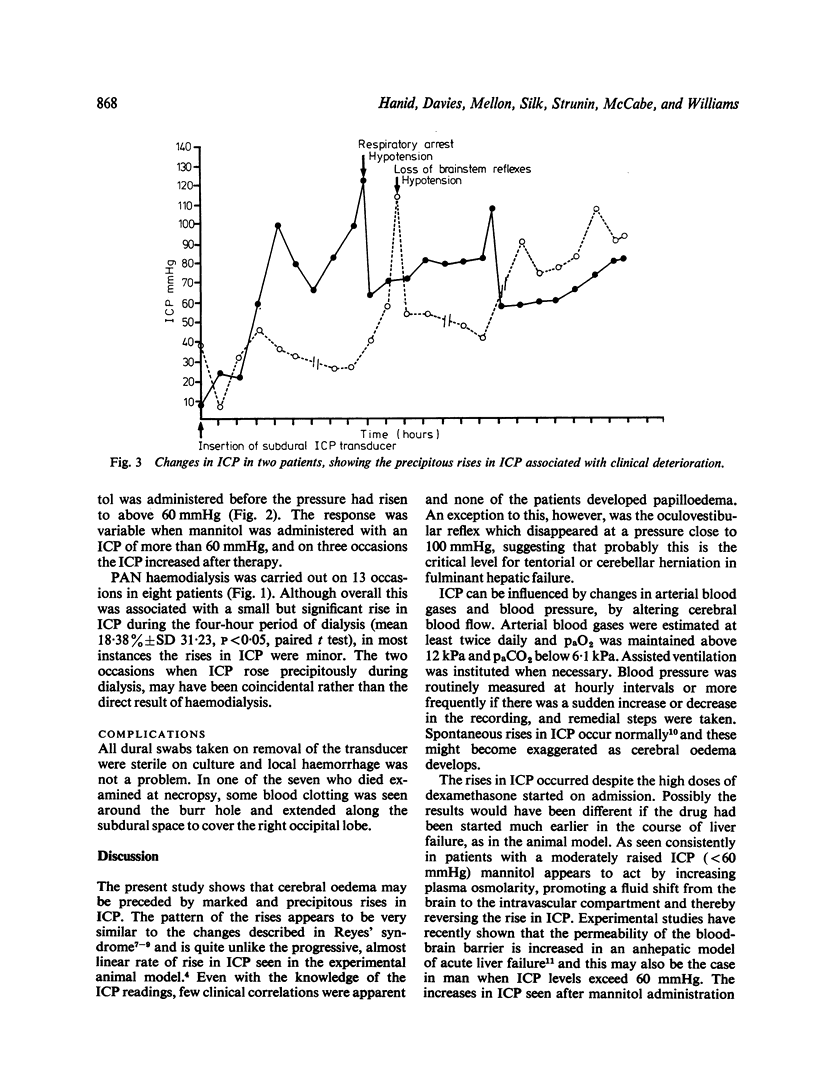
Cerebral oedema is the commonest immediate cause of death in fulminant hepatic failure and an investigation was carried out to determine the value of monitoring intracranial pressure (ICP) and to examine the effects of ICP of dexamethasone therapy and mannitol administration. ICP values in 10 patients at the time of insertion of a subdural pressure transducer (grade IV encephalopathy) averaged 15.5 +/- SD 14.8 mmHg. Despite dexamethansone therapy, which had been started on admission, rises in ICP were subsequently observed in seven of the eight patients who died. In the two patients who survived, the highest reading were 47 and 35 mmHg. Mannitol consistently reversed or arrested ICP rises when pressure was < 60 mmHg. ICP monitoring provides additional information in the managment of patients and is essential if mannitol therapy is to be used.
Full text
PDF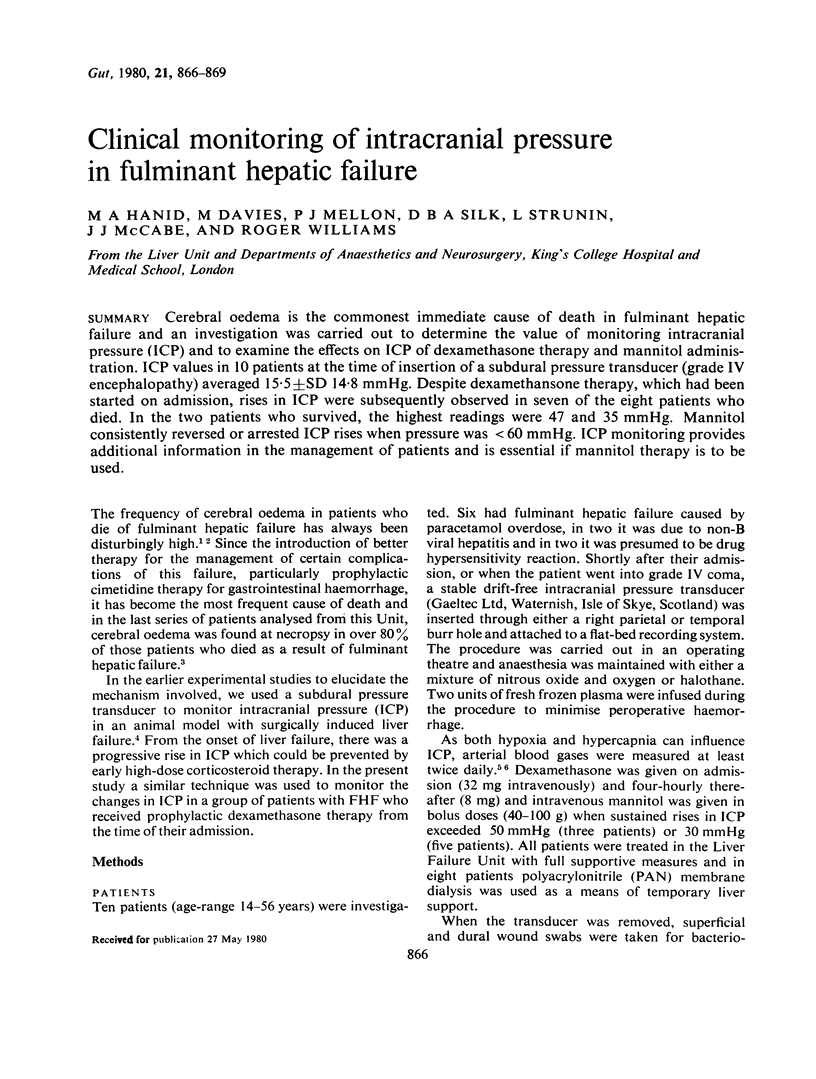

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Gazzard B. G., Portmann B., Murray-Lyon I. M., Williams R. Causes of death in fulminant hepatic failure and relationship to quantitative histological assessment of parenchymal damage. Q J Med. 1975 Oct;44(176):615–626. [PubMed] [Google Scholar]
- Hanid M. A., Mackenzie R. L., Jenner R. E., Chase R. A., Mellon P. J., Trewby P. N., Janota I., Davis M., Silk D. B., Williams R. Intracranial pressure in pigs with surgically induced acute liver failure. Gastroenterology. 1979 Jan;76(1):123–131. [PubMed] [Google Scholar]
- Kindt G. W., Waldman J., Kohl S., Baublis J., Tucker R. P. Intracranial pressure in Reye syndrome. Monitoring and control. JAMA. 1975 Feb 24;231(8):822–825. [PubMed] [Google Scholar]
- Livingstone A. S., Potvin M., Goresky C. A., Finlayson M. H., Hinchey E. J. Changes in the blood-brain barrier in hepatic coma after hepatectomy in the rat. Gastroenterology. 1977 Oct;73(4 Pt 1):697–704. [PubMed] [Google Scholar]
- Mchedlishvili G., Kapuściński A., Nikolaishvili L. Mechanisms of postischemic brain edema: contribution of circulatory factors. Stroke. 1976 Jul-Aug;7(4):410–416. doi: 10.1161/01.str.7.4.410. [DOI] [PubMed] [Google Scholar]
- Mickell J. J., Reigel D. H., Cook D. R., Binda R. E., Safar P. Intracranial pressure: monitoring and normalization therapy in children. Pediatrics. 1977 Apr;59(4):606–613. [PubMed] [Google Scholar]
- Shaywitz B. A., Leventhal J. M., Kramer M. S., Venes J. L. Prolonged continuous monitoring of intracranial pressure in severe Reye's syndrome. Pediatrics. 1977 Apr;59(4):595–605. [PubMed] [Google Scholar]
- Silk D. B., Trewby P. N., Chase R. A., Mellon P. J., Hanid M. A., Davies M., Langley P. G., Wheeler P. G., Williams R. Treatment of fulminant hepatic failure by polyacrylonitrile-membrane haemodialysis. Lancet. 1977 Jul 2;2(8027):1–3. doi: 10.1016/s0140-6736(77)90001-0. [DOI] [PubMed] [Google Scholar]
- Ware A. J., D'Agostino A. N., Combes B. Cerebral edema: a major complication of massive hepatic necrosis. Gastroenterology. 1971 Dec;61(6):877–884. [PubMed] [Google Scholar]