

Abstract
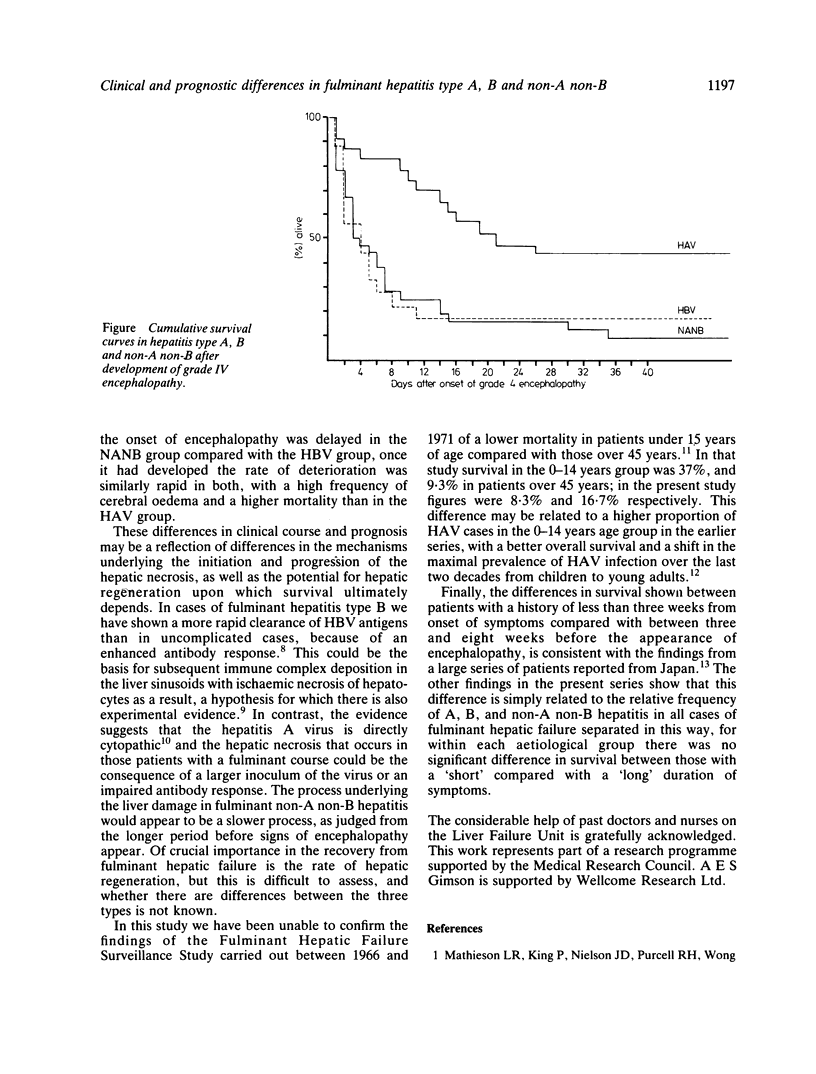
In 73 patients with fulminant viral hepatitis, non-A non-B hepatitis (NANB) was most common (43.8%), with hepatitis type A (HAV) diagnosed in 31.5% and hepatitis type B (HBV) in 24.7%. The non-A non-B group had a significantly longer duration from the onset of symptoms to the appearance of encephalopathy (median 21 days) compared with the HAV and HBV groups (medians 10 and seven days, p less than 0.01 and p less than 0.005 respectively). In the HAV group the severity of liver damage, judged by the maximum prolongation of the prothrombin time, was significantly less than in the HBV group (58 and 150 seconds prolonged respectively, p less than 0.005), and cerebral oedema was significantly less frequent (39% and 72% respectively, p less than 0.05). Consistent with this, the survival rate was higher in the HAV group (43.4%) compared with the HBV group (16.6%) and NANB group (9.3%) (p less than 0.005). These variations in presentation and clinical course may be a consequence of differences in the pathogenesis of the hepatic necrosis.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Boughton C. R. Viral hepatitis in Sydney: a review of fatal illnesses in a hospital series. Med J Aust. 1968 Aug 24;2(8):343–350. doi: 10.5694/j.1326-5377.1968.tb82821.x. [DOI] [PubMed] [Google Scholar]
- Farrow L. J., Stewart J. S., Stern H., Clifford R. E., Smith H. G., Zuckerman A. J. Non-A, non-B hepatitis in West London. Lancet. 1981 May 2;1(8227):982–984. doi: 10.1016/s0140-6736(81)91741-4. [DOI] [PubMed] [Google Scholar]
- Mori W. The Shwartzman reaction: a review including clinical manifestations and proposal for a univisceral or single organ third type. Histopathology. 1981 Mar;5(2):113–126. doi: 10.1111/j.1365-2559.1981.tb01772.x. [DOI] [PubMed] [Google Scholar]
- Rakela J., Redeker A. G., Edwards V. M., Decker R., Overby L. R., Mosley J. W. Hepatits A virus infection in fulminant hepatitis and chronic active hepatitis. Gastroenterology. 1978 May;74(5 Pt 1):879–882. [PubMed] [Google Scholar]
- Rueff B., Benhamou J. P. Acute hepatic necrosis and fulminant hepatic failure. Gut. 1973 Oct;14(10):805–815. doi: 10.1136/gut.14.10.805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tedder R. S., Wilson-Croome R. Detection by radioimmunoassay of IgM class antibody to hepatitis B core antigen: a comparison of two methods. J Med Virol. 1980;6(3):235–247. doi: 10.1002/jmv.1890060307. [DOI] [PubMed] [Google Scholar]
- Trey C. The fulminant hepatic failure surveillance study. Brief review of the effects of presumed etiology and age of survival. Can Med Assoc J. 1972 Feb 26;106:525–528. [PMC free article] [PubMed] [Google Scholar]