

Abstract
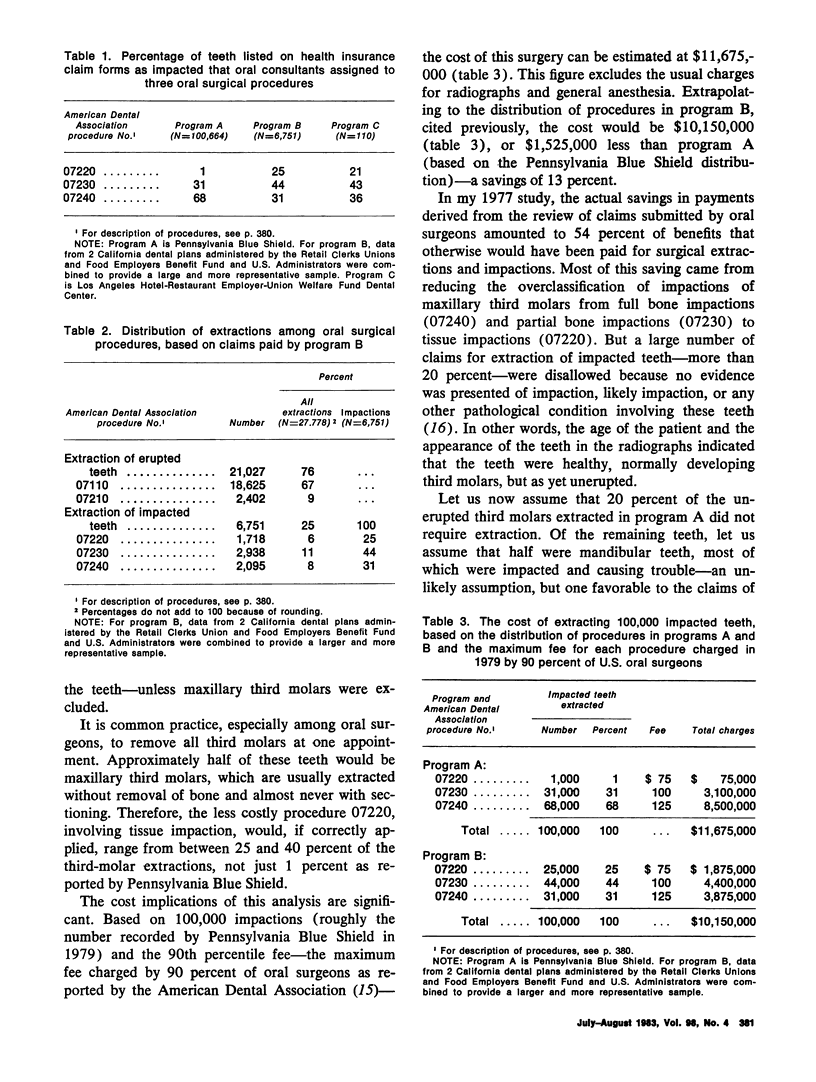
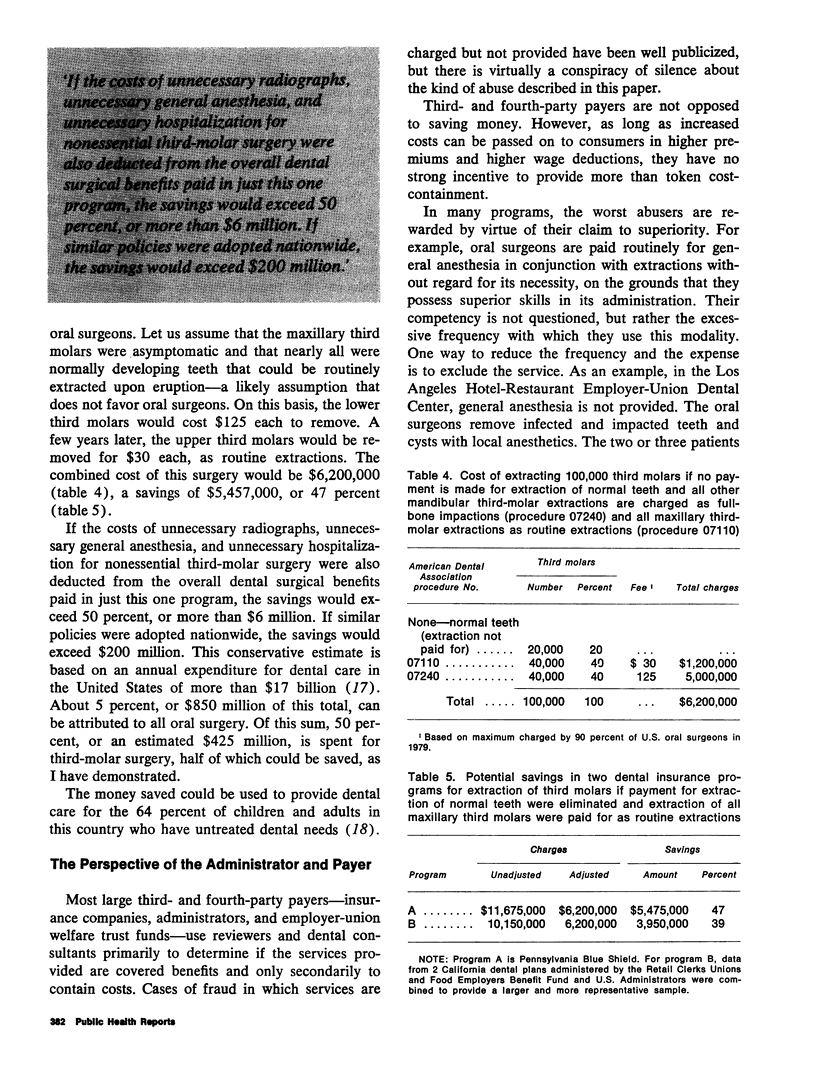
No known scientific studies support the extraction of third molars (wisdom teeth) to prevent future disease. Yet, third-molar surgery for this purpose has become so common that in at least one major U.S. health insurance plan, the cumulative cost exceeds that for every other kind of major surgery. Many third molars that are developing normally in adolescents are classified as impacted and removed before they erupt, a practice that results in large expenditures for unnecessary surgery. In addition, the difficulty of the extractions is frequently exaggerated, so that patients and insurance plans are overcharged. Third molar surgery is not without risk of iatrogenic injury. Fracture of the jaw, permanent numbness of the lip (paresthesia), and injury to other teeth may occur. This paper presents a mechanism for containing the cost of third-molar surgery by elimination of payment for nonessential extractions and of the related overcharges. Adoption of this policy by administrators of dental insurance plans would save millions of dollars each year, money that could be better used in providing care for more people with real dental disease.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BHASKAR S. N. ADENOAMELOBLASTOMA: ITS HISTOGENESIS AND REPORT OF 15 NEW CASES. J Oral Surg Anesth Hosp Dent Serv. 1964 May;22:218–226. [PubMed] [Google Scholar]
- Beideman R. W., Johnson O. N., Alcox R. W. A study to develop a rating system and evaluate dental radiographs submitted to a third party carrier. J Am Dent Assoc. 1976 Nov;93(5):1010–1013. doi: 10.14219/jada.archive.1976.0037. [DOI] [PubMed] [Google Scholar]
- Chretien P. B., Carpenter D. F., White N. S., Harrah J. D., Lightbody P. M. Squamous carcinoma arising in a dentigerous cyst. Presentation of a fatal case and review of four previously reported cases. Oral Surg Oral Med Oral Pathol. 1970 Dec;30(6):809–816. doi: 10.1016/0030-4220(70)90345-2. [DOI] [PubMed] [Google Scholar]
- Clark H. L. Retention of nonpathologic impacted, embedded, or nonfunctioning third molars. J Mass Dent Soc. 1982 Spring;31(2):72–73. [PubMed] [Google Scholar]
- DACHI S. F., HOWELL F. V. A survey of 3, 874 routine full-month radiographs. II. A study of impacted teeth. Oral Surg Oral Med Oral Pathol. 1961 Oct;14:1165–1169. doi: 10.1016/0030-4220(61)90204-3. [DOI] [PubMed] [Google Scholar]
- FRANK V. H. Paresthesia: evaluation of 16 cases. J Oral Surg Anesth Hosp Dent Serv. 1959 Nov;17:27–33. [PubMed] [Google Scholar]
- Friedman J. W. PSROs in dentistry. Am J Public Health. 1975 Dec;65(12):1298–1303. doi: 10.2105/ajph.65.12.1298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman J. W. The case for preservation of third molars. CDA J. 1977 Feb;5(2):50–56. [PubMed] [Google Scholar]
- Kaplan R. G. Mandibular third molars and postretention crowding. Am J Orthod. 1974 Oct;66(4):411–430. doi: 10.1016/0002-9416(74)90050-5. [DOI] [PubMed] [Google Scholar]
- Kipp D. P., Goldstein B. H., Weiss W. W., Jr Dysesthesia after mandibular third molar surgery: a retrospective study and analysis of 1,377 surgical procedures. J Am Dent Assoc. 1980 Feb;100(2):185–192. doi: 10.14219/jada.archive.1980.0074. [DOI] [PubMed] [Google Scholar]
- Rud J. The split-bone technic for removal of impacted mandibular third molars. J Oral Surg. 1970 Jun;28(6):416–421. [PubMed] [Google Scholar]
- STANLEY H. R., DIEHL D. L. AMELOBLASTOMA POTENTIAL OF FOLLICULAR CYSTS. Oral Surg Oral Med Oral Pathol. 1965 Aug;20:260–268. doi: 10.1016/0030-4220(65)90200-8. [DOI] [PubMed] [Google Scholar]