

Abstract
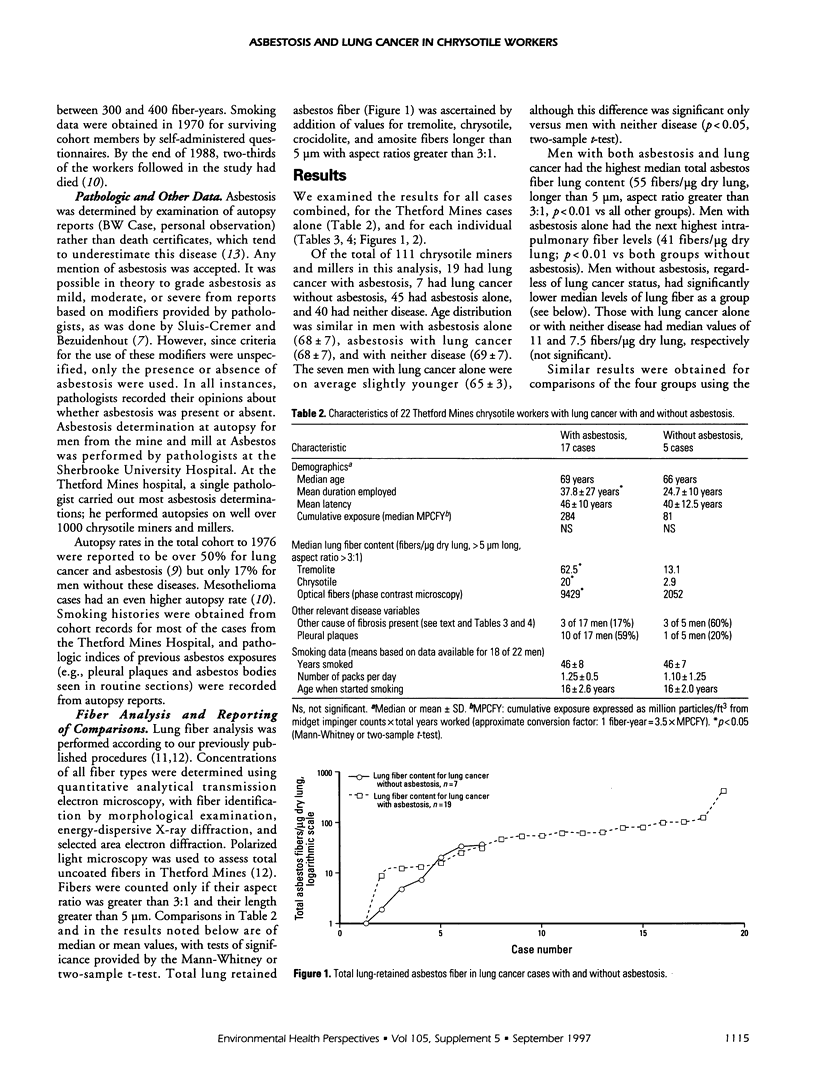
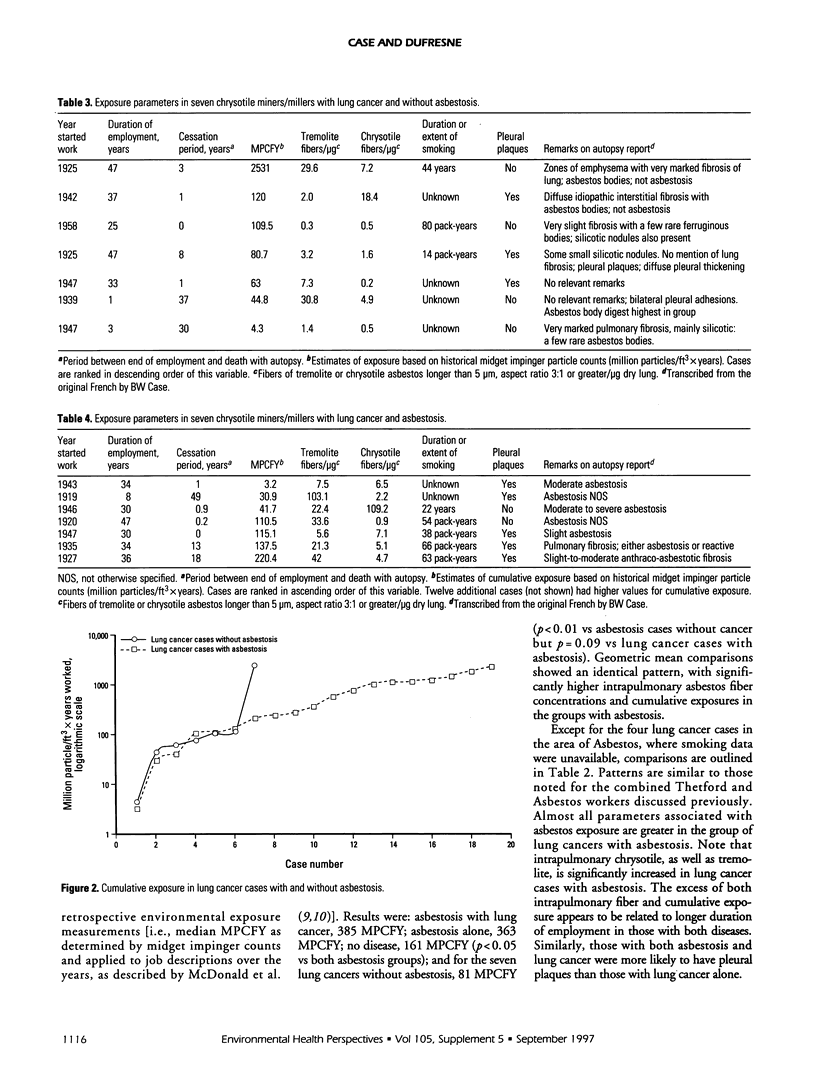
One prospective epidemiologic study of asbestos cement workers with radiological small opacities has been cited as a rationale for attributing excess lung cancer to asbestosis. This approach could have considerable practical value for disease attribution in an era of decreasing exposure. However, a recent International Agency for Research on Cancer review concludes that the mechanism of production of asbestos-related lung cancer are unknown. Asbestosis, therefore, cannot be a biologically effective dose marker of lung cancer susceptibility. Asbestosis nonetheless would be useful in identifying asbestos-attributable lung cancer cases if it could be proven an infallible exposure indicator. In this study, we tested this hypothesis in the chrysotile miners and millers of Quebec, Canada. We examined exposure histories, autopsy records, and lung fiber content for 111 Quebec chrysotile miners and millers. If the hypothesis of an asbestosis requirement for lung cancer attribution were accurate, we would expect as asbestosis diagnosis to separate those with lung cancer and high levels of exposure from those with lower levels of exposure in a specific and sensitive manner. This is the first such study in which historical job-based individual estimates based on environmental measurements, lung fiber content, exposure timing, and complete pathology records including autopsies were available for review. We found significant excesses of lung tremolite and chrysotile and estimated cumulative exposure in those with lung cancer and asbestosis compared to those with lung cancer without asbestosis. However, when the latter were directly compared on a case-by-case basis, there was a marked overlap between lung cancer cases with and without asbestosis regardless of the measure of exposure. Smoking habits did not differ between lung cancer cases with and without asbestosis. In regression models, smoking pack-years discriminated between those with the without lung cancer, regardless of asbestosis status. Most seriously, the pathologic diagnosis of asbestosis itself seemed arbitrary in many cases. We conclude that although the presence of pathologically diagnosed asbestosis is a useful marker of exposure, the absence of this disease must be regarded as one of many factors in determining individual exposure status and disease causation.
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Abraham J. L. Asbestos inhalation, not asbestosis, causes lung cancer. Am J Ind Med. 1994 Dec;26(6):839–842. doi: 10.1002/ajim.4700260614. [DOI] [PubMed] [Google Scholar]
- Case B. W. Biological indicators of chrysotile exposure. Ann Occup Hyg. 1994 Aug;38(4):503-18, 410-1. doi: 10.1093/annhyg/38.4.503. [DOI] [PubMed] [Google Scholar]
- Case B. W., Sebastien P. Environmental and occupational exposures to chrysotile asbestos: a comparative microanalytic study. Arch Environ Health. 1987 Jul-Aug;42(4):185–191. [PubMed] [Google Scholar]
- Egilman D., Reinert A. Lung cancer and asbestos exposure: asbestosis is not necessary. Am J Ind Med. 1996 Oct;30(4):398–406. doi: 10.1002/(SICI)1097-0274(199610)30:4<398::AID-AJIM4>3.0.CO;2-S. [DOI] [PubMed] [Google Scholar]
- Hughes J. M., Weill H. Asbestosis as a precursor of asbestos related lung cancer: results of a prospective mortality study. Br J Ind Med. 1991 Apr;48(4):229–233. doi: 10.1136/oem.48.4.229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kipen H. M., Lilis R., Suzuki Y., Valciukas J. A., Selikoff I. J. Pulmonary fibrosis in asbestos insulation workers with lung cancer: a radiological and histopathological evaluation. Br J Ind Med. 1987 Feb;44(2):96–100. doi: 10.1136/oem.44.2.96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDonald J. C., Liddell F. D., Dufresne A., McDonald A. D. The 1891-1920 birth cohort of Quebec chrysotile miners and millers: mortality 1976-88. Br J Ind Med. 1993 Dec;50(12):1073–1081. doi: 10.1136/oem.50.12.1073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDonald J. C., Liddell F. D., Gibbs G. W., Eyssen G. E., McDonald A. D. Dust exposure and mortality in chrysotile mining, 1910-75. Br J Ind Med. 1980 Feb;37(1):11–24. doi: 10.1136/oem.37.1.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roggli V. L., Hammar S. P., Pratt P. C., Maddox J. C., Legier J., Mark E. J., Brody A. R. Does asbestos or asbestosis cause carcinoma of the lung? Am J Ind Med. 1994 Dec;26(6):835–838. doi: 10.1002/ajim.4700260613. [DOI] [PubMed] [Google Scholar]
- Sebastien P., McDonald J. C., McDonald A. D., Case B., Harley R. Respiratory cancer in chrysotile textile and mining industries: exposure inferences from lung analysis. Br J Ind Med. 1989 Mar;46(3):180–187. doi: 10.1136/oem.46.3.180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sluis-Cremer G. K., Bezuidenhout B. N. Relation between asbestosis and bronchial cancer in amphibole asbestos miners. Br J Ind Med. 1989 Aug;46(8):537–540. doi: 10.1136/oem.46.8.537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilkinson P., Hansell D. M., Janssens J., Rubens M., Rudd R. M., Taylor A. N., McDonald C. Is lung cancer associated with asbestos exposure when there are no small opacities on the chest radiograph? Lancet. 1995 Apr 29;345(8957):1074–1078. doi: 10.1016/s0140-6736(95)90817-x. [DOI] [PubMed] [Google Scholar]