

Abstract
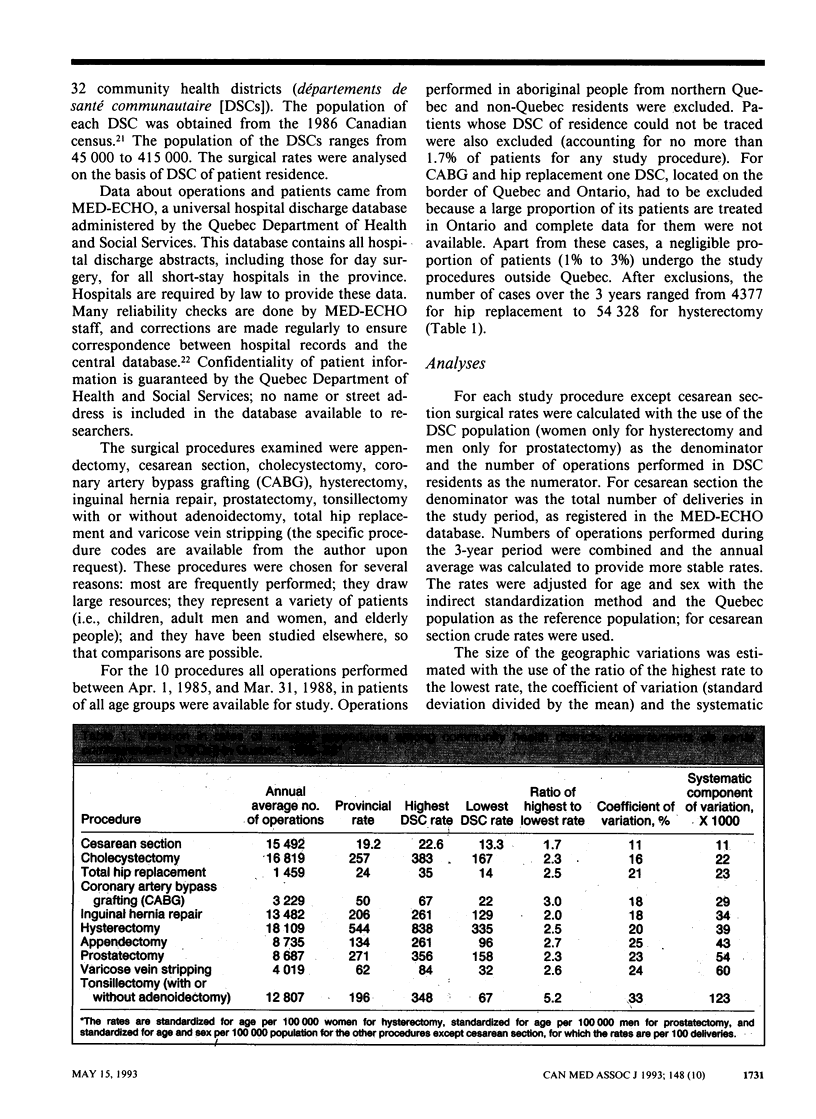
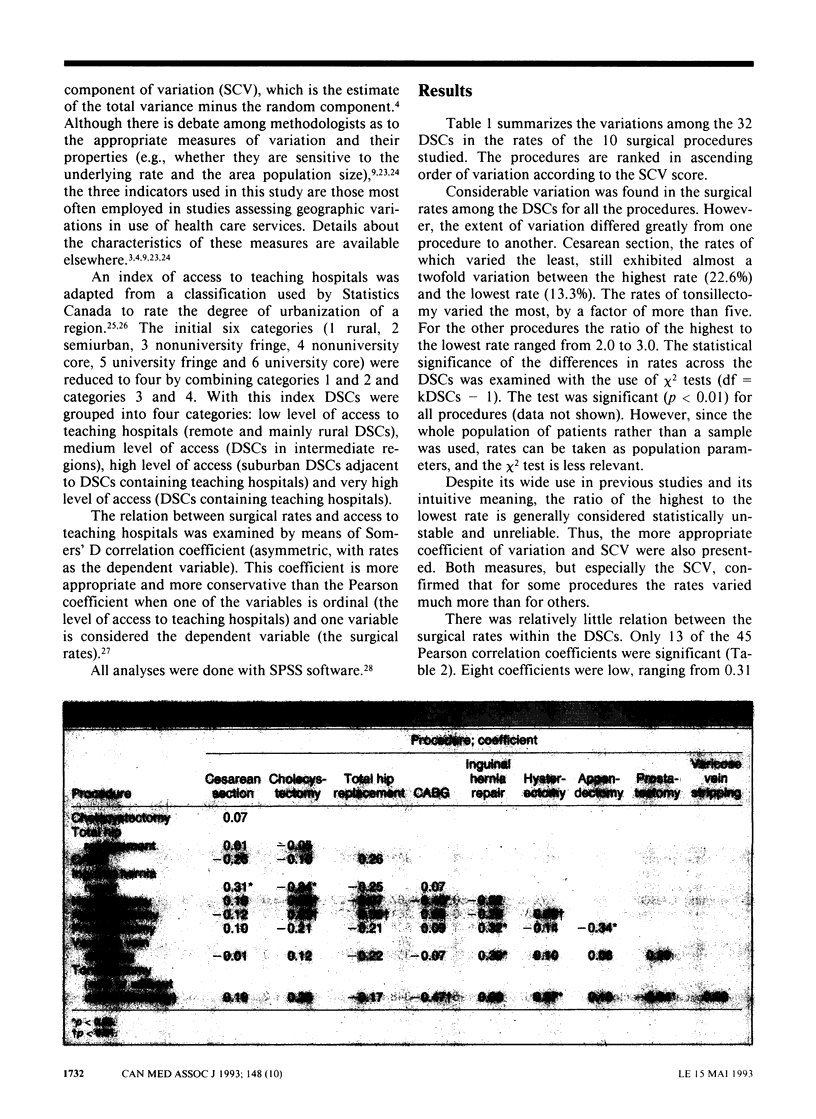
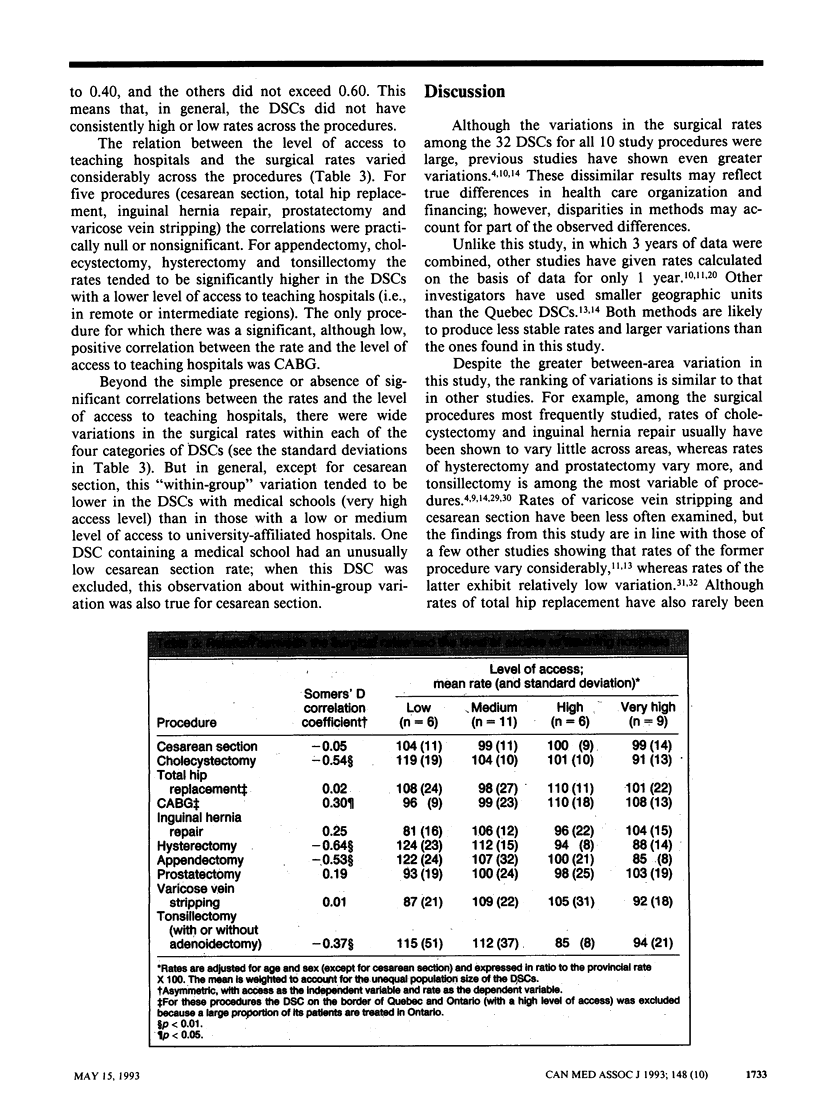
OBJECTIVE: To document the geographic variations in the rates of 10 common surgical procedures in Quebec and to examine the relation between surgical rates and level of access to teaching hospitals. DESIGN: Population-based rates standardized for age and sex were calculated from 1985-88 data from MED-ECHO (the provincial hospital discharge database) for each of the 32 community health districts (départements de santé communautaire [DSCs]) in Quebec. Variation across DSCs was analysed with the use of the ratio of the highest to the lowest rate, the coefficient of variation and the systematic component of variation. On the basis of an urbanization index designed by Statistics Canada, DSCs were classified as having a low, medium, high or very high level of access to teaching hospitals. PATIENTS: All Quebec residents except those whose DSC of residence could not be traced (accounting for no more than 1.7% of patients for any study procedure) and aboriginal people from northern Quebec. SURGICAL PROCEDURES STUDIED: Appendectomy, cesarean section, cholecystectomy, coronary artery bypass grafting (CABG), hysterectomy, inguinal hernia repair, prostatectomy, tonsillectomy with or without adenoidectomy, total hip replacement and varicose vein stripping. RESULTS: There was considerable systematic variation in the surgical rates for all 10 procedures. Cesarean section, the rates of which varied the least, still exhibited almost a twofold variation between the highest and lowest rates. The rates of tonsillectomy varied the most, by a factor of more than five. With a few exceptions there was relatively little relation between the rates of the procedures within the DSCs. The rates of appendectomy, cholecystectomy, hysterectomy and tonsillectomy tended to be lower in the DSCs containing teaching hospitals, whereas the reverse was true for CABG. For the other procedures the relation between the rates and the level of access to teaching hospitals was nonsignificant. CONCLUSIONS: The overall consistency of the observed variations with those of previous studies invites a closer look at the practice patterns and the scientific basis of the clinical decisions associated with procedures showing high variations in rates. The lack of a systematic relation between the surgical rates and the level of access to teaching hospitals challenges the belief that remote regions are underserved with respect to the procedures studied.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anderson G. M., Lomas J. Explaining variations in cesarean section rates: patients, facilities or policies? Can Med Assoc J. 1985 Feb 1;132(3):253-6, 259. [PMC free article] [PubMed] [Google Scholar]
- Black N. Geographical variations in use of surgery for glue ear. J R Soc Med. 1985 Aug;78(8):641–648. doi: 10.1177/014107688507800809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bunker J. P. Surgical manpower. A comparison of operations and surgeons in the United States and in England and Wales. N Engl J Med. 1970 Jan 15;282(3):135–144. doi: 10.1056/NEJM197001152820306. [DOI] [PubMed] [Google Scholar]
- Chassin M. R., Brook R. H., Park R. E., Keesey J., Fink A., Kosecoff J., Kahn K., Merrick N., Solomon D. H. Variations in the use of medical and surgical services by the Medicare population. N Engl J Med. 1986 Jan 30;314(5):285–290. doi: 10.1056/NEJM198601303140505. [DOI] [PubMed] [Google Scholar]
- Clark J. D. Variation in Michigan hospital use rates: do physician and hospital characteristics provide the explanation? Soc Sci Med. 1990;30(1):67–82. doi: 10.1016/0277-9536(90)90330-u. [DOI] [PubMed] [Google Scholar]
- Detmer D. E., Tyron T. J. Delivery of surgical care: inferences based on hospital discharge abstract data. Surg Forum. 1976;27(62):460–463. [PubMed] [Google Scholar]
- Diehr P., Cain K. C., Kreuter W., Rosenkranz S. Can small-area analysis detect variation in surgery rates? The power of small-area variation analysis. Med Care. 1992 Jun;30(6):484–502. doi: 10.1097/00005650-199206000-00003. [DOI] [PubMed] [Google Scholar]
- Diehr P., Cain K., Connell F., Volinn E. What is too much variation? The null hypothesis in small-area analysis. Health Serv Res. 1990 Feb;24(6):741–771. [PMC free article] [PubMed] [Google Scholar]
- Dyck F. J., Murphy F. A., Murphy J. K., Road D. A., Boyd M. S., Osborne E., De Vlieger D., Korchinski B., Ripley C., Bromley A. T. Effect of surveillance on the number of hysterectomies in the province of Saskatchewan. N Engl J Med. 1977 Jun 9;296(23):1326–1328. doi: 10.1056/NEJM197706092962306. [DOI] [PubMed] [Google Scholar]
- Lewis C. E. Variations in the incidence of surgery. N Engl J Med. 1969 Oct 16;281(16):880–884. doi: 10.1056/NEJM196910162811606. [DOI] [PubMed] [Google Scholar]
- McMahon L. F., Jr, Wolfe R. A., Tedeschi P. J. Variation in hospital admissions among small areas. A comparison of Maine and Michigan. Med Care. 1989 Jun;27(6):623–631. doi: 10.1097/00005650-198906000-00005. [DOI] [PubMed] [Google Scholar]
- McPherson K., Wennberg J. E., Hovind O. B., Clifford P. Small-area variations in the use of common surgical procedures: an international comparison of New England, England, and Norway. N Engl J Med. 1982 Nov 18;307(21):1310–1314. doi: 10.1056/NEJM198211183072104. [DOI] [PubMed] [Google Scholar]
- Mindell W. R., Vayda E., Cardillo B. Ten-year trends in Canada for selected operations. Can Med Assoc J. 1982 Jul 1;127(1):23–27. [PMC free article] [PubMed] [Google Scholar]
- Naylor C. D., Ugnat A. M., Weinkauf D., Anderson G. M., Wielgosz A. Coronary artery bypass grafting in Canada: What is its rate of use? Which rate is right? CMAJ. 1992 Mar 15;146(6):851–859. [PMC free article] [PubMed] [Google Scholar]
- Pearson R. J., Smedby B., Berfenstam R., Logan R. F., Burgess A. M., Jr, Peterson O. L. Hospital caseloads in Liverpool, New England, and Uppsala. An international comparison. Lancet. 1968 Sep 7;2(7567):559–566. doi: 10.1016/s0140-6736(68)92423-9. [DOI] [PubMed] [Google Scholar]
- Phelps C. E., Parente S. T. Priority setting in medical technology and medical practice assessment. Med Care. 1990 Aug;28(8):703–723. doi: 10.1097/00005650-199008000-00004. [DOI] [PubMed] [Google Scholar]
- Roos N. P. Hysterectomy: variations in rates across small areas and across physicians' practices. Am J Public Health. 1984 Apr;74(4):327–335. doi: 10.2105/ajph.74.4.327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roos N. P., Roos L. L., Jr, Henteleff P. D. Elective surgical rates--do high rates mean lower standards? Tonsillectomy and adenoidectomy in Manitoba. N Engl J Med. 1977 Aug 18;297(7):360–365. doi: 10.1056/NEJM197708182970705. [DOI] [PubMed] [Google Scholar]
- Roos N. P., Roos L. L., Jr Surgical rate variations: do they reflect the health or socioeconomic characteristics of the population? Med Care. 1982 Sep;20(9):945–958. doi: 10.1097/00005650-198209000-00007. [DOI] [PubMed] [Google Scholar]
- Roos N. P., Wennberg J. E., McPherson K. Using diagnosis-related groups for studying variations in hospital admissions. Health Care Financ Rev. 1988 Summer;9(4):53–62. [PMC free article] [PubMed] [Google Scholar]
- Simpson A. Variations in operation rates in New Zealand. N Z Med J. 1986 Oct 22;99(812):798–801. [PubMed] [Google Scholar]
- Vayda E. A comparison of surgical rates in Canada and in England and Wales. N Engl J Med. 1973 Dec 6;289(23):1224–1229. doi: 10.1056/NEJM197312062892305. [DOI] [PubMed] [Google Scholar]
- Vayda E., Anderson G. D. Comparison of provincial surgical rates in 1968. Can J Surg. 1975 Jan;18(1):18-9, 22-6. [PubMed] [Google Scholar]
- Vayda E., Barnsley J. M., Mindell W. R., Cardillo B. Five-year study of surgical rates in Ontario's counties. Can Med Assoc J. 1984 Jul 15;131(2):111–115. [PMC free article] [PubMed] [Google Scholar]
- Vayda E., Mindell W. R., Rutkow I. M. A decade of surgery in Canada, England and Wales, and the United States. Arch Surg. 1982 Jun;117(6):846–853. doi: 10.1001/archsurg.1982.01380300086019. [DOI] [PubMed] [Google Scholar]
- Vayda E., Morison M., Anderson G. D. Surgical rates in the Canadian provinces, 1968 to 1972. Can J Surg. 1976 May;19(3):235–242. [PubMed] [Google Scholar]
- Wennberg J. E., Barnes B. A., Zubkoff M. Professional uncertainty and the problem of supplier-induced demand. Soc Sci Med. 1982;16(7):811–824. doi: 10.1016/0277-9536(82)90234-9. [DOI] [PubMed] [Google Scholar]
- Wennberg J. E. Dealing with medical practice variations: a proposal for action. Health Aff (Millwood) 1984 Summer;3(2):6–32. doi: 10.1377/hlthaff.3.2.6. [DOI] [PubMed] [Google Scholar]
- Wennberg J. E., Fowler F. J., Jr A test of consumer contribution to small area variations in health care delivery. J Maine Med Assoc. 1977 Aug;68(8):275–279. [PubMed] [Google Scholar]
- Wennberg J. E., Freeman J. L., Culp W. J. Are hospital services rationed in New Haven or over-utilised in Boston? Lancet. 1987 May 23;1(8543):1185–1189. doi: 10.1016/s0140-6736(87)92152-0. [DOI] [PubMed] [Google Scholar]
- Wennberg J. E., McPherson K., Caper P. Will payment based on diagnosis-related groups control hospital costs? N Engl J Med. 1984 Aug 2;311(5):295–300. doi: 10.1056/NEJM198408023110505. [DOI] [PubMed] [Google Scholar]
- Wennberg J., Gittelsohn Small area variations in health care delivery. Science. 1973 Dec 14;182(4117):1102–1108. doi: 10.1126/science.182.4117.1102. [DOI] [PubMed] [Google Scholar]