

Abstract
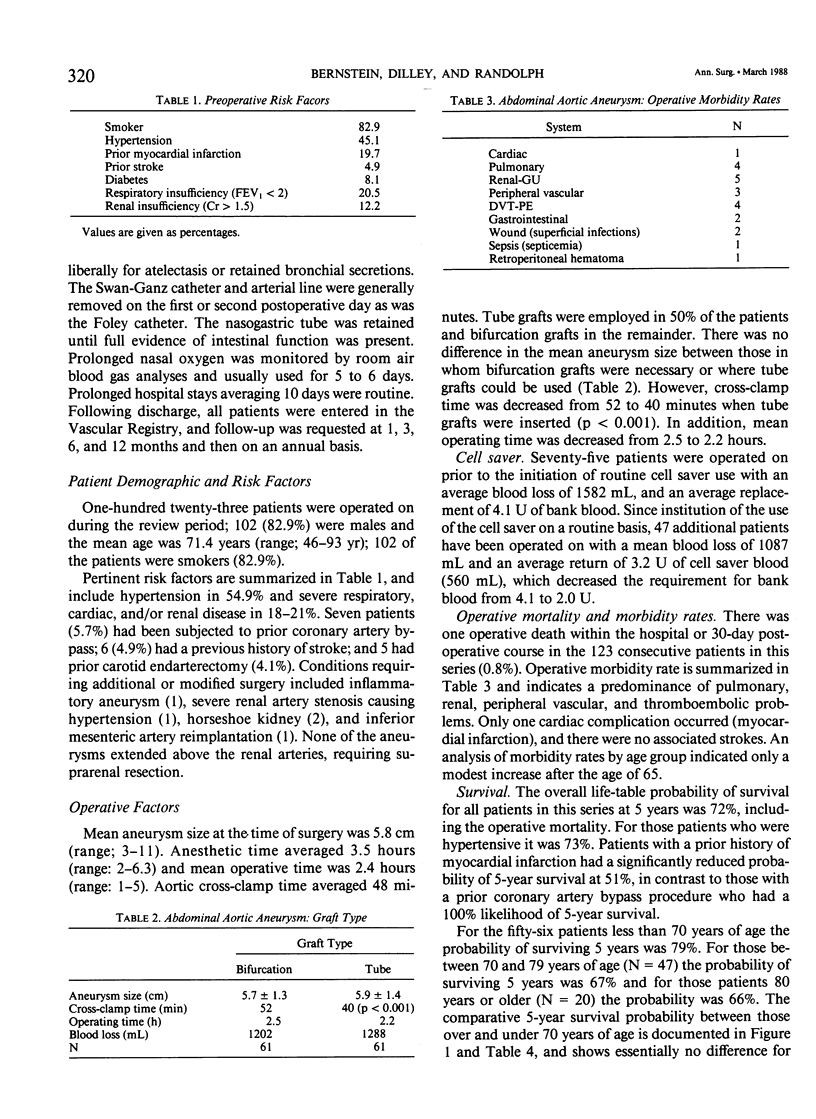
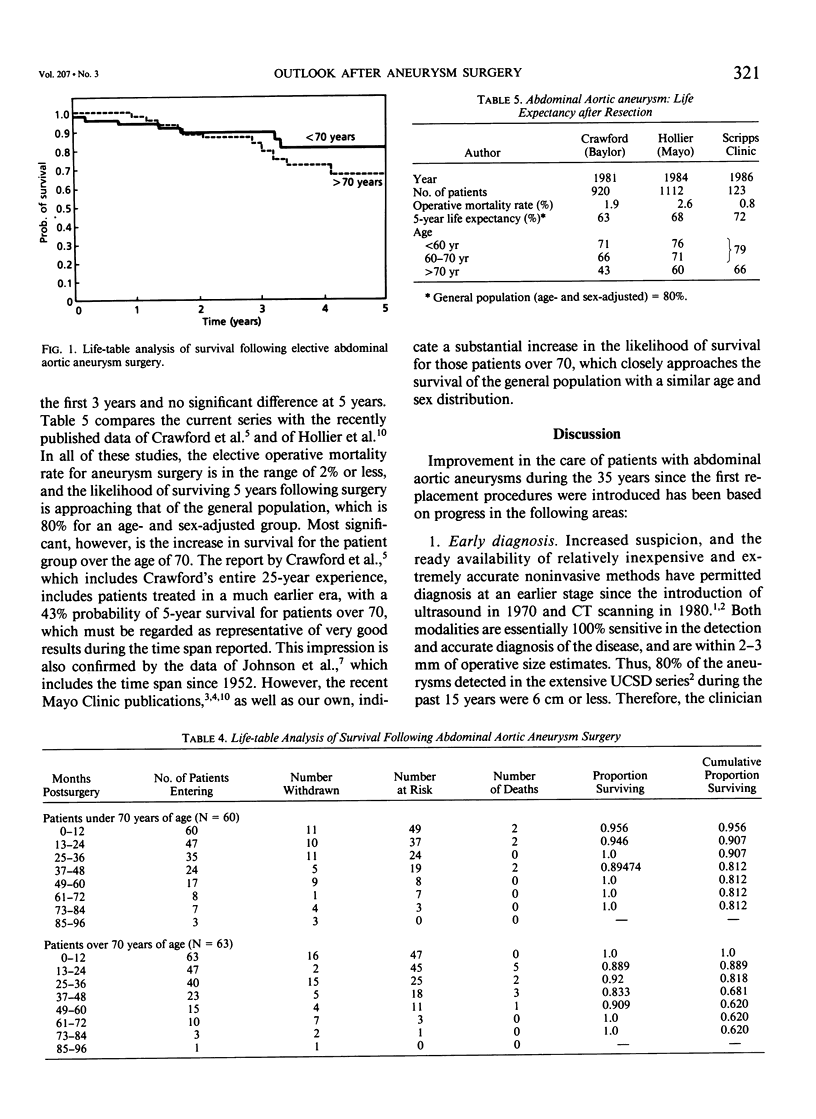
During the past decade, selective criteria for elective surgery for abdominal aortic aneurysms have been refined based on natural history and aneurysm expansion information. Using these criteria, contemporary preoperative preparation and newer intraoperative technical adjuncts, 123 consecutive patients underwent elective resection with 1 death (mortality rate: 0.8%). These include all patients operated on with both elective and urgent aneurysms at this institution since 1978, with the exception of those with frank rupture. Most importantly, however, the 5-year life-table survival of all of these patients (average age: 71.3 years, range 46-96 yr) was 72%, including both hospital and late mortality rates. More than half of the patients were over 70 years old (78 cases), with no hospital deaths and a 5-year life-table survival probability of 67%. For those under 70 years of age at the time of operation, the 5-year life-table probability of survival was 79%. We believe that these accomplishments were a direct result of an aggressive policy of screening for and selectively treating coronary disease and carotid stenosis preoperatively and the utilization of such intraoperative adjuncts as routine Swan-Ganz monitoring, autologous blood transfusion, the cell saver, and the frequent use of the tube grafting (50%). Thus, with proper selection, the outlook for the patient over 70 years old with an elective abdominal aortic aneurysm resection now approaches that of the normal population (67% vs. 69%).
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bernstein E. F., Chan E. L. Abdominal aortic aneurysm in high-risk patients. Outcome of selective management based on size and expansion rate. Ann Surg. 1984 Sep;200(3):255–263. doi: 10.1097/00000658-198409000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernstein E. F., Dilley R. B., Goldberger L. E., Gosink B. B., Leopold G. R. Growth rates of small abdominal aortic aneurysms. Surgery. 1976 Dec;80(6):765–773. [PubMed] [Google Scholar]
- Bickerstaff L. K., Hollier L. H., Van Peenen H. J., Melton L. J., 3rd, Pairolero P. C., Cherry K. J. Abdominal aortic aneurysms: the changing natural history. J Vasc Surg. 1984 Jan;1(1):6–12. [PubMed] [Google Scholar]
- Brown O. W., Hollier L. H., Pairolero P. C., Kazmier F. J., McCready R. A. Abdominal aortic aneurysm and coronary artery disease. Arch Surg. 1981 Nov;116(11):1484–1488. doi: 10.1001/archsurg.1981.01380230098015. [DOI] [PubMed] [Google Scholar]
- Crawford E. S., Saleh S. A., Babb J. W., 3rd, Glaeser D. H., Vaccaro P. S., Silvers A. Infrarenal abdominal aortic aneurysm: factors influencing survival after operation performed over a 25-year period. Ann Surg. 1981 Jun;193(6):699–709. doi: 10.1097/00000658-198106000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GEHAN E. A. A GENERALIZED WILCOXON TEST FOR COMPARING ARBITRARILY SINGLY-CENSORED SAMPLES. Biometrika. 1965 Jun;52:203–223. [PubMed] [Google Scholar]
- Hertzer N. R. Fatal myocardial infarction following abdominal aortic aneurysm resection. Three hundred forty-three patients followed 6--11 years postoperatively. Ann Surg. 1980 Nov;192(5):667–673. doi: 10.1097/00000658-198019250-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hertzer N. R., Young J. R., Kramer J. R., Phillips D. F., deWolfe V. G., Ruschhaupt W. F., 3rd, Beven E. G. Routine coronary angiography prior to elective aortic reconstruction: results of selective myocardial revascularization in patients with peripheral vascular disease. Arch Surg. 1979 Nov;114(11):1336–1344. doi: 10.1001/archsurg.1979.01370350138018. [DOI] [PubMed] [Google Scholar]
- Hollier L. H., Plate G., O'Brien P. C., Kazmier F. J., Gloviczki P., Pairolero P. C., Cherry K. J. Late survival after abdominal aortic aneurysm repair: influence of coronary artery disease. J Vasc Surg. 1984 Mar;1(2):290–299. [PubMed] [Google Scholar]
- Leather R. P., Shah D., Goldman M., Rosenberg M., Karmody A. M. Nonresective treatment of abdominal aortic aneurysms. Use of acute thrombosis and axillofemoral bypass. Arch Surg. 1979 Dec;114(12):1402–1408. doi: 10.1001/archsurg.1979.01370360056006. [DOI] [PubMed] [Google Scholar]
- Ruby S. T., Whittemore A. D., Couch N. P., Collins J. J., Cohn L., Shemin R., Mannick J. A. Coronary artery disease in patients requiring abdominal aortic aneurysm repair. Selective use of a combined operation. Ann Surg. 1985 Jun;201(6):758–764. doi: 10.1097/00000658-198506000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz R. A., Nichols W. K., Silver D. Is thrombosis of the infrarenal abdominal aortic aneurysm an acceptable alternative? J Vasc Surg. 1986 Mar;3(3):448–455. doi: 10.1067/mva.1986.avs0030448. [DOI] [PubMed] [Google Scholar]
- Whittemore A. D., Clowes A. W., Hechtman H. B., Mannick J. A. Aortic aneurysm repair. Reduced operative mortality associated with maintenance of optimal cardiac performance. Ann Surg. 1980 Sep;192(3):414–421. doi: 10.1097/00000658-198009000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]