

Abstract
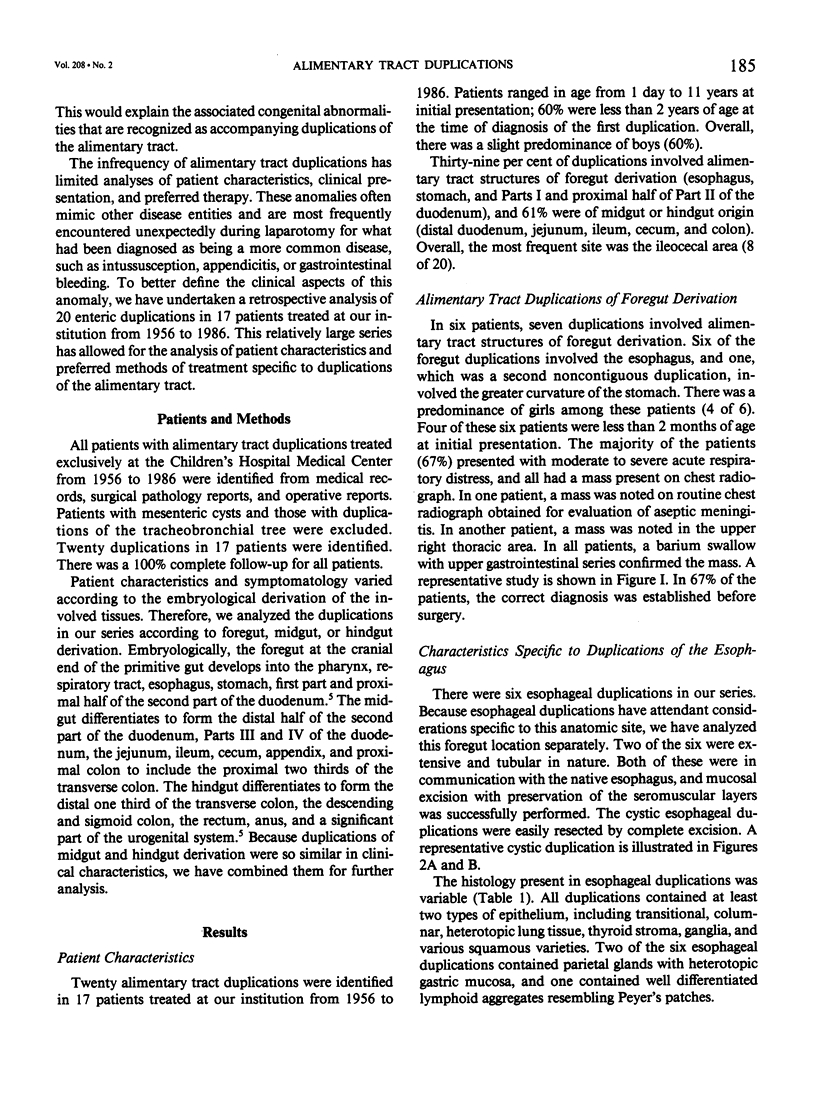
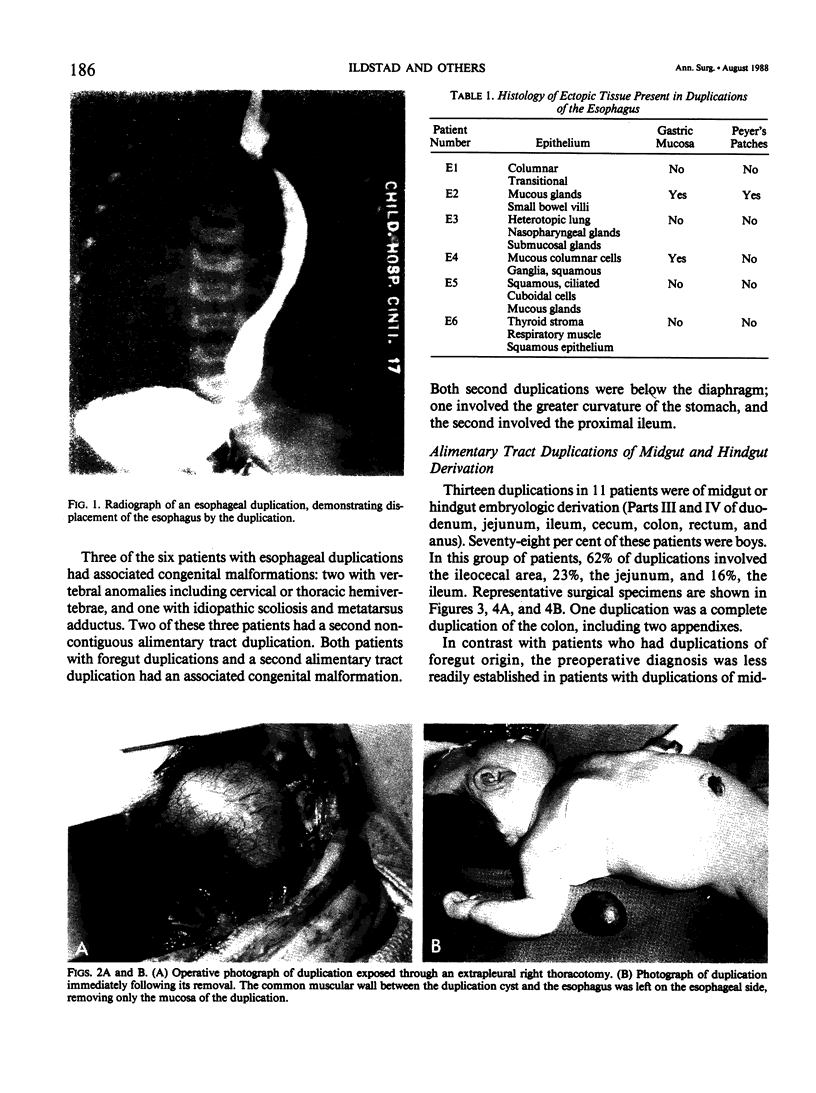
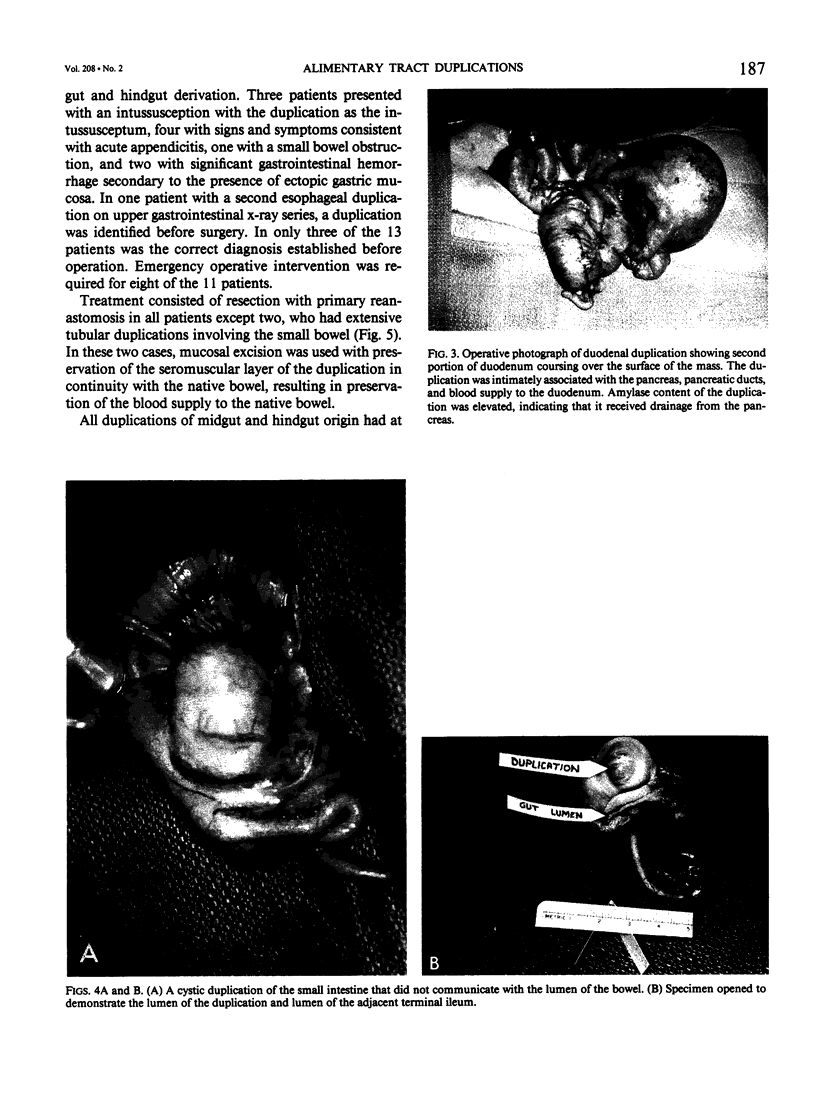
Duplications of the alimentary tract are unusual congenital anomalies that frequently present a diagnostic as well as therapeutic challenge to the surgeon. Because these lesions occur so infrequently, they are often not suspected until encountered intraoperatively. Due to the complicated anatomy and common blood supply shared between the duplication and associated native bowel, appropriate management requires a familiarity with the anatomy and clinical characteristics of this entity. To better define the range of patient characteristics, clinical presentation, and preferred therapy, 20 enteric duplications were reviewed in 17 patients treated at the Children's Hospital Medical Center from 1956 to 1986. Ages of patients ranged from 1 day to 11 years; 60% were less than 2 years of age at initial presentation. Seven duplications in six patients involved alimentary tract structures of foregut derivation (esophagus, stomach, and Parts I and II of duodenum), with a predominance of girls (4 of 6). Most of these patients (67%) presented with moderate to severe acute respiratory distress and a mass present on chest radiograph. In 67% of the patients, the correct diagnosis was established before operation. None required emergency operative intervention. By contrast, 13 duplications in 11 patients were of midgut or hindgut derivation (Parts III and IV of the duodenum, jejunum, ileum, and colon). In this group of patients, 62% of the duplications involved the cecum, 23% involved the ileum, and 16%, the jejunum. Seventy-eight per cent of the patients were boys. The most common symptoms were nausea and vomiting, and the most common sign was a palpable abdominal mass. Emergency operative intervention was required of eight of 11 patients with duplications involving the small bowel and colon. Three patients presented with an intussusception, four with signs and symptoms consistent with acute appendicitis, one with a small bowel obstruction, and two with gastrointestinal hemorrhage due to the presence of ectopic gastric mucosa within the duplication. It was found that two important points must be considered in regard to the management of enteric duplications: (1) the common blood supply shared between the duplication and native bowel must be carefully protected to avoid undue sacrifice of normal bowel, and (2) the presence of heterotopic gastric mucosa in 35% of patients negates internal drainage.(ABSTRACT TRUNCATED AT 400 WORDS)
Full text
PDF


Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Knight J., Garvin P. J., Lewis E., Jr Gastric duplication presenting as a double esophagus. J Pediatr Surg. 1983 Jun;18(3):300–301. doi: 10.1016/s0022-3468(83)80110-9. [DOI] [PubMed] [Google Scholar]
- LEWIS P. L., HOLDER T., FELDMAN M. Duplication of the stomach. Report of a case and review of the English literature. Arch Surg. 1961 Apr;82:634–640. doi: 10.1001/archsurg.1961.01300100148017. [DOI] [PubMed] [Google Scholar]
- MELLISH R. W., KOOP C. E. Clinical manifestations of duplication of the bowel. Pediatrics. 1961 Mar;27:397–407. [PubMed] [Google Scholar]
- WRENN E. L., Jr Tubular duplication of the small intestine. Surgery. 1962 Sep;52:494–498. [PubMed] [Google Scholar]