

Abstract
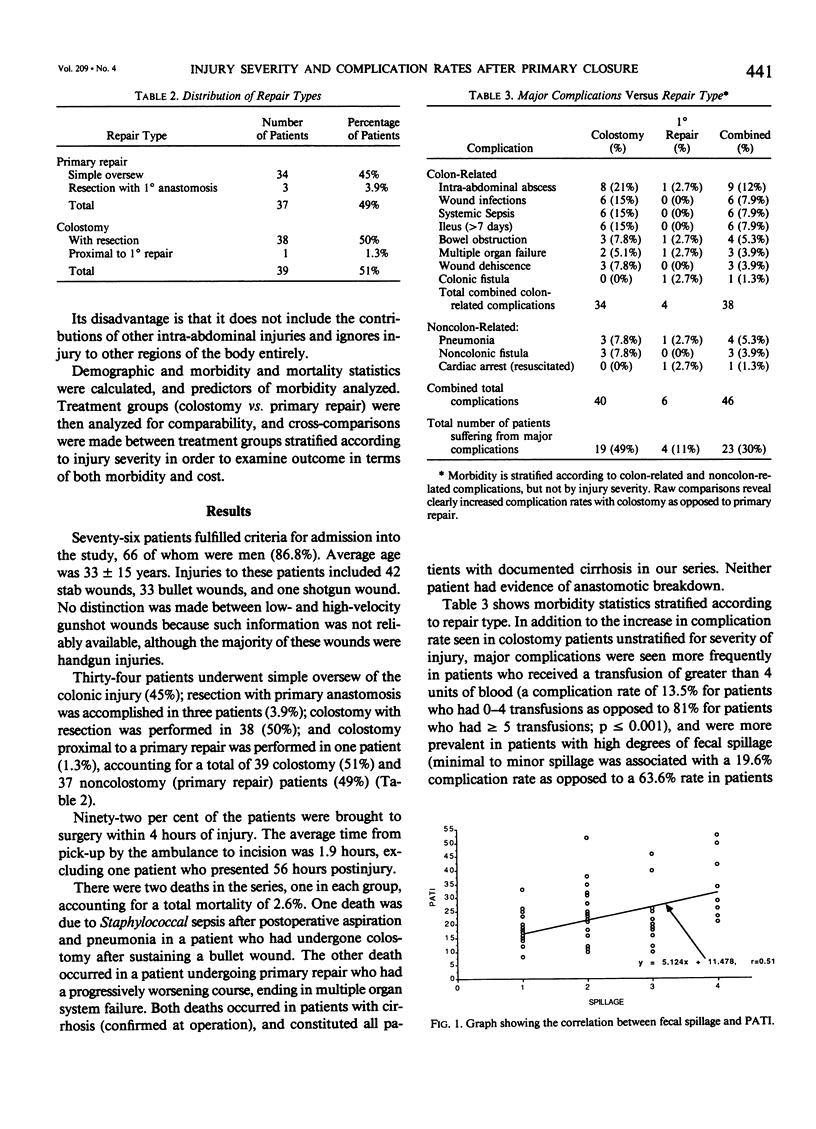
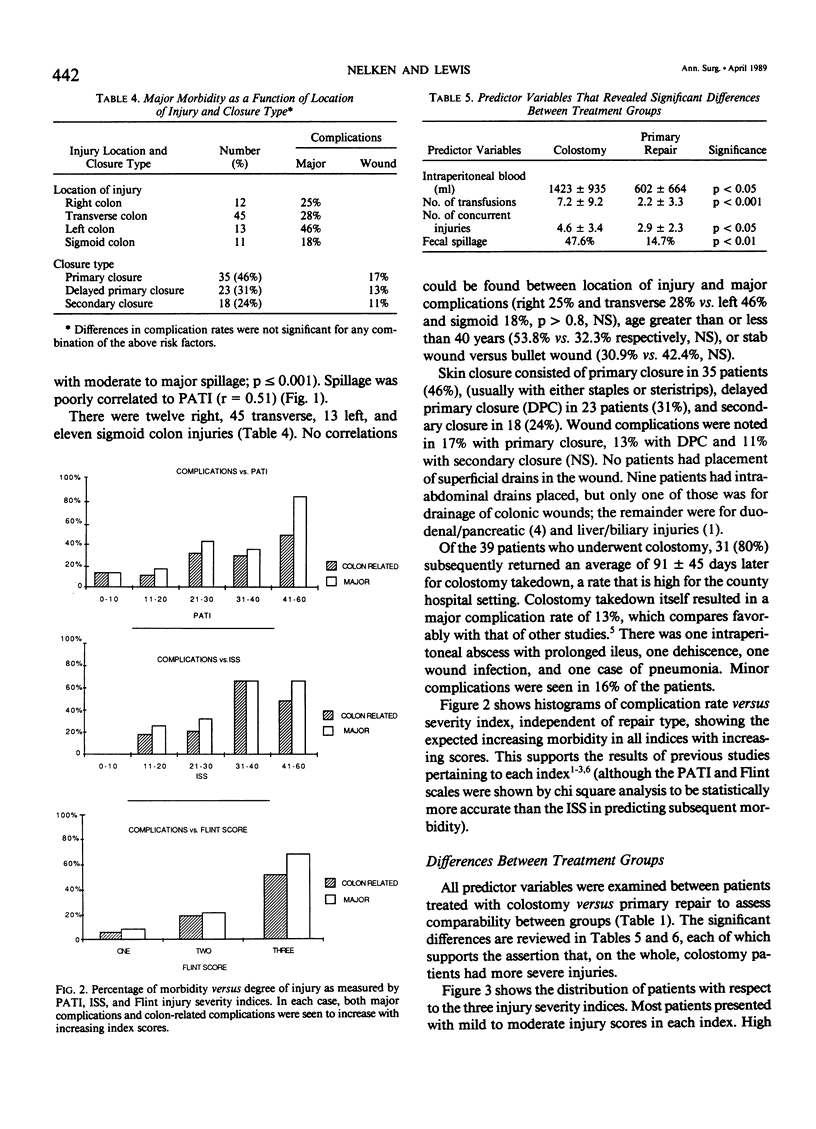
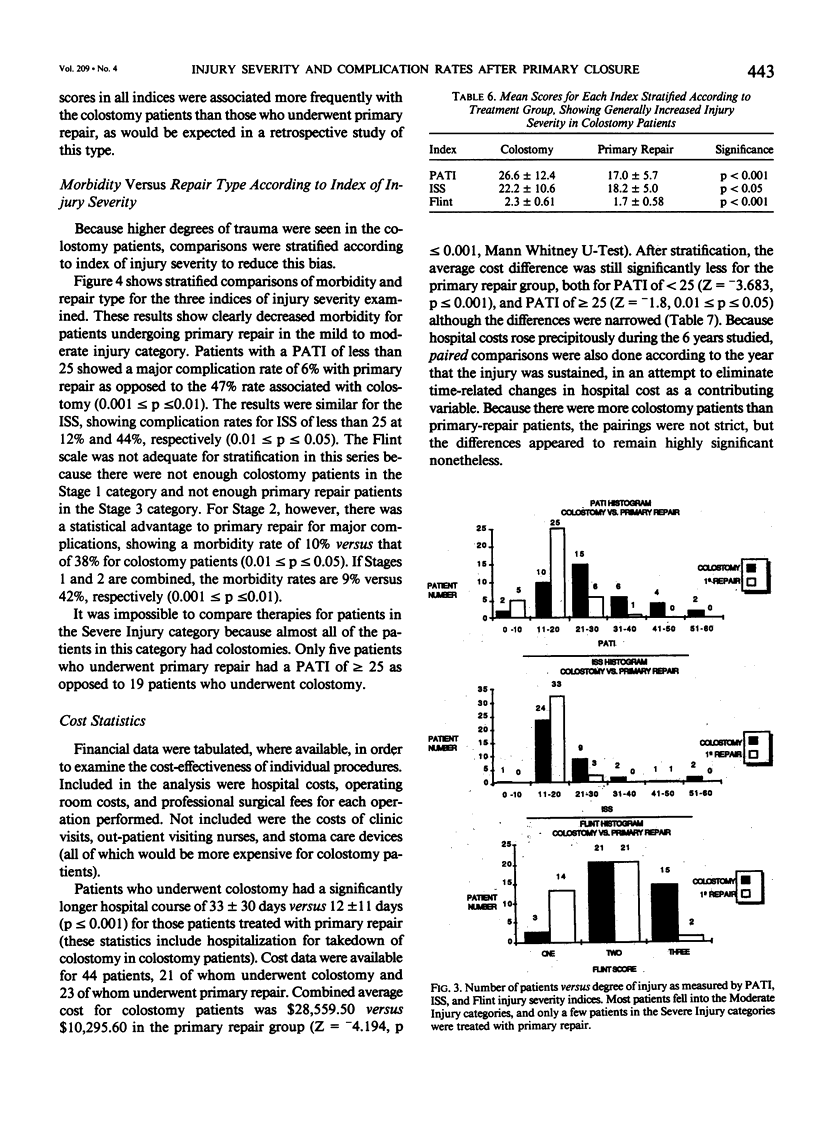
The management of penetrating colon injury has been frequently debated in the literature, yet few reports have evaluated primary closure versus diverting colostomy in similarly injured patients. Diverting colostomy is the standard of care when mucosal penetration is present, but primary closure in civilian practice has generally had excellent results, although it has been restricted to less severely injured patients. Because the degree of injury may influence choice of treatment in modern practice, various indices of injury severity have been proposed for assessment of patients with penetrating colon trauma. As yet, however, there has been no cross-comparison of repair type versus injury severity. A retrospective study 76 patients who sustained penetrating colon trauma between January 1, 1979 and December 31, 1985 and who survived for at least 24 hours was conducted. Different preferences among attending surgeons and a more aggressive approach to the use of primary closure during the years of study led to an essentially random use of primary closure and diverting colostomy for moderate levels of colon injury, with mandatory colostomy reserved for the most serious injuries. Primary closure was performed in 37 patients (three having resection and anastomosis), and colostomy was performed in 39 patients. Severity of injury was evaluated by the Injury Severity Score (ISS), Penetrating Abdominal Trauma Index (PATI), and the Flint Colon Injury Score. Complications and outcome were evaluated as a function of severity of injury, and primary closure and colostomy were compared. Demographic profiles of the two groups did not differ regarding age, sex, mechanism of injury, shock, or delay between injury and operation. The mortality rate was 2.6% for each group. Major morbidity, including septic complications, occurred in 11% of the patients of the primary closure group and in 49% of those of the colostomy group. When PATI was less than 25, the Flint score was less than or equal to 2, or when the ISS was less than 25, primary closure resulted in fewer complications than did colostomy. Of the injury severity indices examined, the PATI most reliably predicted complications and specifically identified patients who whose outcome would be good with primary repair. These results suggest that the use of primary closure should be expanded in civilian penetrating colon trauma and that, even with moderate degrees of colon injury, primary closure provides an outcome equivalent to that provided by colostomy. In addition, the predictive value of the PATI suggests that it should be included along with other injury severity indices in trauma data bases.
Full text
PDF


Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Adkins R. B., Jr, Zirkle P. K., Waterhouse G. Penetrating colon trauma. J Trauma. 1984 Jun;24(6):491–499. doi: 10.1097/00005373-198406000-00006. [DOI] [PubMed] [Google Scholar]
- Baker S. P., O'Neill B., Haddon W., Jr, Long W. B. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974 Mar;14(3):187–196. [PubMed] [Google Scholar]
- Crass R. A., Salbi F., Trunkey D. D. Colostomy closure after colon injury: a low-morbidity procedure. J Trauma. 1987 Nov;27(11):1237–1239. doi: 10.1097/00005373-198711000-00008. [DOI] [PubMed] [Google Scholar]
- Dang C. V., Peter E. T., Parks S. N., Ellyson J. H. Trauma of the colon: early drop-back of exteriorized repair. Arch Surg. 1982 May;117(5):652–656. doi: 10.1001/archsurg.1982.01380290098017. [DOI] [PubMed] [Google Scholar]
- Dellinger E. P., Oreskovich M. R., Wertz M. J., Hamasaki V., Lennard E. S. Risk of infection following laparotomy for penetrating abdominal injury. Arch Surg. 1984 Jan;119(1):20–27. doi: 10.1001/archsurg.1984.01390130010002. [DOI] [PubMed] [Google Scholar]
- Demetriades D., Rabinowitz B., Sofianos C., Prümm E. The management of colon injuries by primary repair or colostomy. Br J Surg. 1985 Nov;72(11):881–883. doi: 10.1002/bjs.1800721110. [DOI] [PubMed] [Google Scholar]
- Flint L. M., Vitale G. C., Richardson J. D., Polk H. C., Jr The injured colon: relationships of management to complications. Ann Surg. 1981 May;193(5):619–623. doi: 10.1097/00000658-198105000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karanfilian R. G., Ghuman S. S., Pathak V. B., Swaminathan A. P., Machiedo G. W., Blackwood J. M. Penetrating injuries to the colon. Am Surg. 1982 Mar;48(3):103–108. [PubMed] [Google Scholar]
- LoCicero J., 3rd, Tajima T., Drapanas T. A half-century of experience in the management of colon injuries: changing concepts. J Trauma. 1975 Jul;15(7):575–579. doi: 10.1097/00005373-197507000-00003. [DOI] [PubMed] [Google Scholar]
- Moore E. E., Dunn E. L., Moore J. B., Thompson J. S. Penetrating abdominal trauma index. J Trauma. 1981 Jun;21(6):439–445. [PubMed] [Google Scholar]
- Panton O. N., Atkinson K. G., Crichton E. P., Schulzer M., Beaufoy A., Germann E. Mechanical preparation of the large bowel for elective surgery. Comparison of whole-gut lavage with the conventional enema and purgative technique. Am J Surg. 1985 May;149(5):615–619. doi: 10.1016/s0002-9610(85)80139-2. [DOI] [PubMed] [Google Scholar]
- Schrock T. R., Christensen N. Management of perforating injuries of the colon. Surg Gynecol Obstet. 1972 Jul;135(1):65–68. [PubMed] [Google Scholar]
- Shannon F. L., Moore E. E. Primary repair of the colon: when is it a safe alternative? Surgery. 1985 Oct;98(4):851–860. [PubMed] [Google Scholar]
- Stone H. H., Fabian T. C. Management of perforating colon trauma: randomization between primary closure and exteriorization. Ann Surg. 1979 Oct;190(4):430–436. doi: 10.1097/00000658-197910000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thal E. R., Yeary E. C. Morbidity of colostomy closure following colon trauma. J Trauma. 1980 Apr;20(4):287–291. doi: 10.1097/00005373-198004000-00003. [DOI] [PubMed] [Google Scholar]
- Thompson J. S., Moore E. E. Factors affecting the outcome of exteriorized colon repairs. J Trauma. 1982 May;22(5):403–406. doi: 10.1097/00005373-198205000-00009. [DOI] [PubMed] [Google Scholar]
- WOODHALL J. P., OCHSNER A. The management of perforating injuries of the colon and rectum in civilian practice. Surgery. 1951 Feb;29(2):305–320. [PubMed] [Google Scholar]