

Abstract
A number of acute and chronic inflammatory disorders are amenable to varying degrees of therapeutic control with the administration of nonspecific anti-inflammatory drugs. An evaluation of these suppressive agents in the field of rheumatic diseases and practical suggestions regarding their administration are presented.
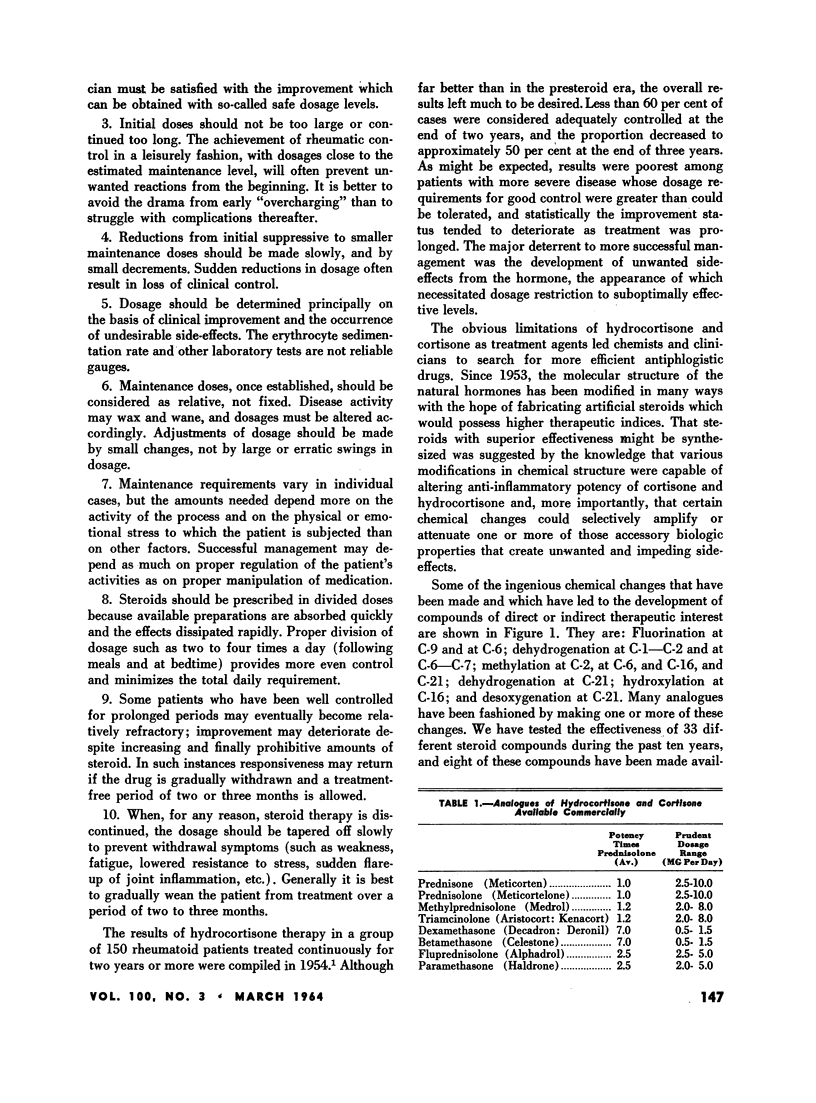
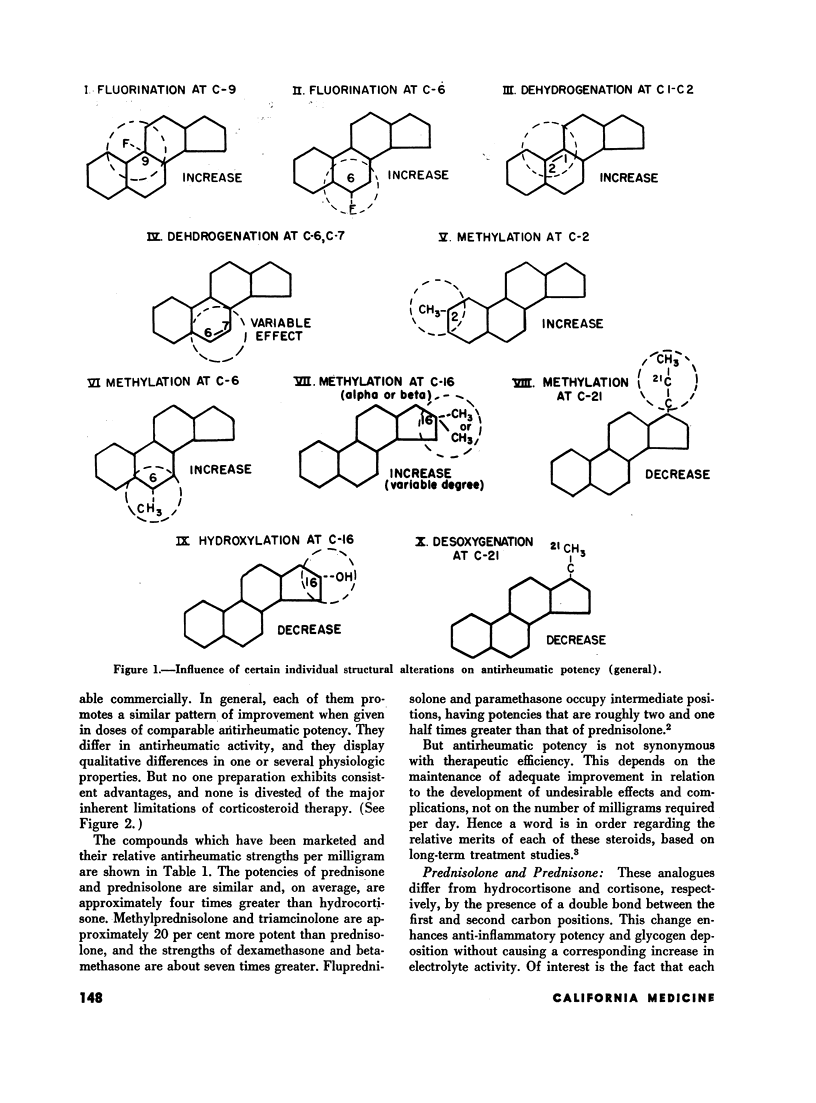
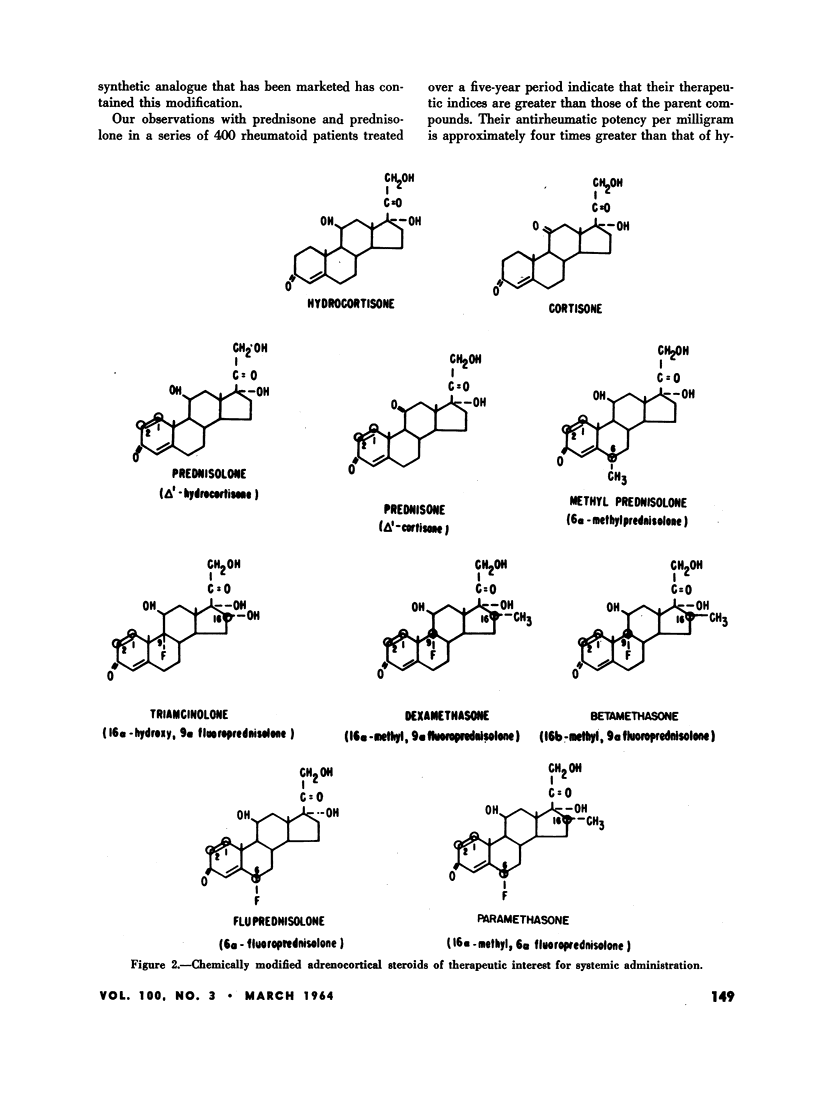
Eight synthetically modified corticosteroid compounds are available commercially. Each of them exhibits qualitative differences in one or several physiologic actions, each has certain advantages and disadvantages in therapy, and each shares the major deterrent features of corticosteroids. Prednisone, prednisolone, methylprednisolone, fluprednisolone and paramethasone have similar therapeutic indices, and there is little choice between them for the usual rheumatoid patient requiring steroid therapy. Conversely, the therapeutic indices of dexamethasone, betamethasone and triamcinolone are lower than that of prednisolone; they are less desirable for routine use and should be reserved for specially selected cases.
Salicylates are preferred to adrenocortical steroids in the treatment of the ordinary patient with acute rheumatic fever. Steroid therapy should be reserved for resistant cases and for those with significant carditis. Salicylates are mainstays for pain relief in rheumatoid arthritis, but with the analgesic doses usually employed their anti-inflammatory action is slight.
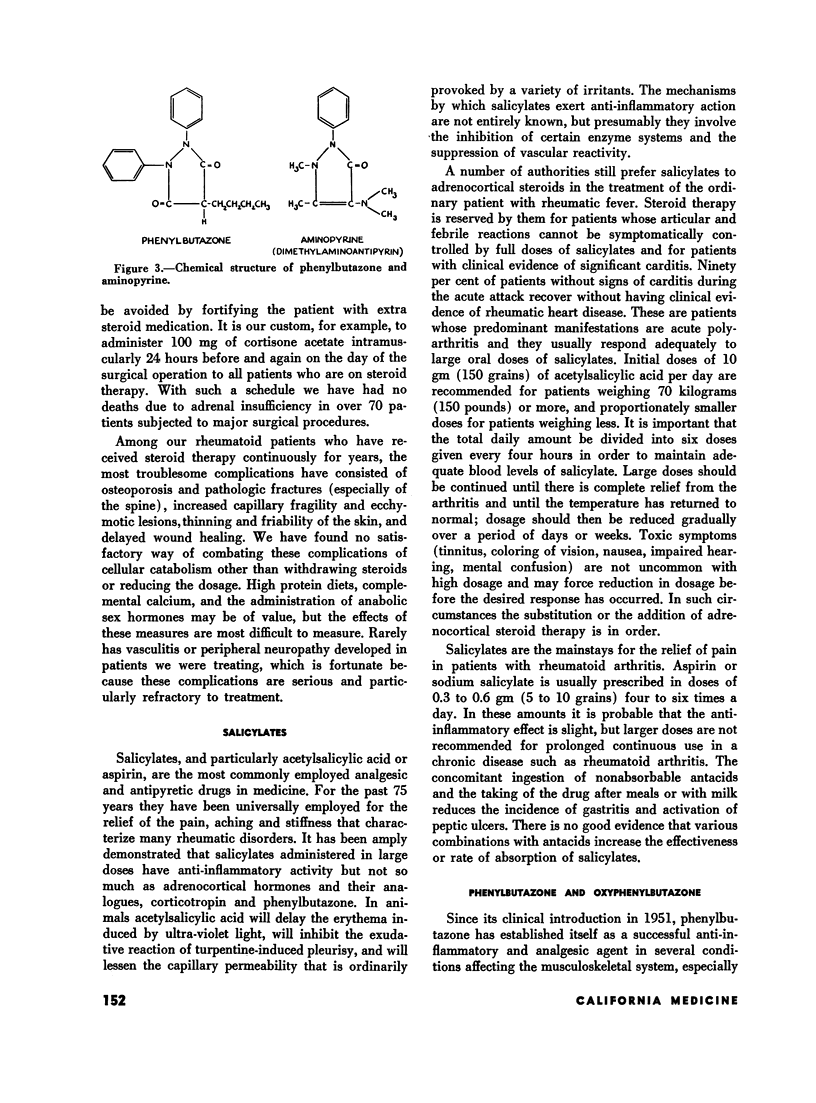
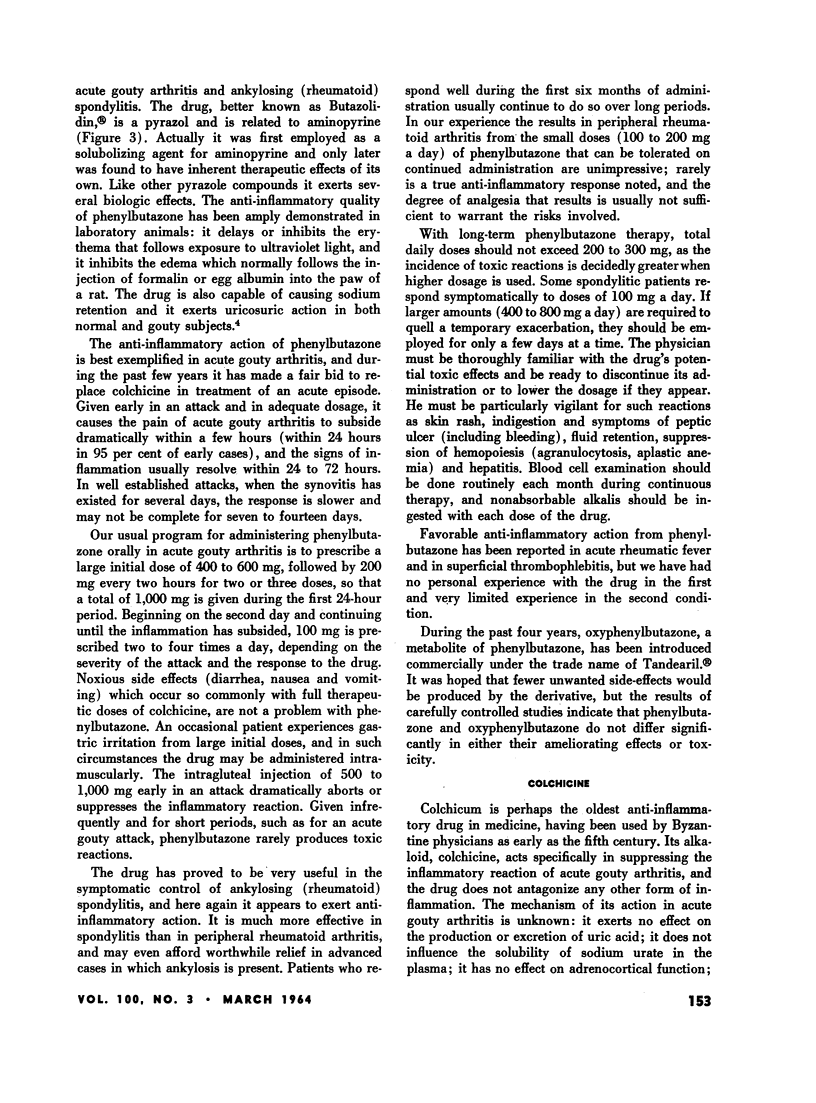
Phenylbutazone is a highly useful anti-inflammatory agent, especially in management of acute gouty arthritis and ankylosing (rheumatoid) spondylitis; its metabolite, oxyphenylbutazone, does not exhibit clear-cut advantages.
Colchicine specifically suppresses acute gouty arthritis. Its analogues, desacetylcolchicine and desacetylthiocolchicine, produce fewer unpleasant gastrointestinal symptoms, but may promote agranulocytosis and alopecia.
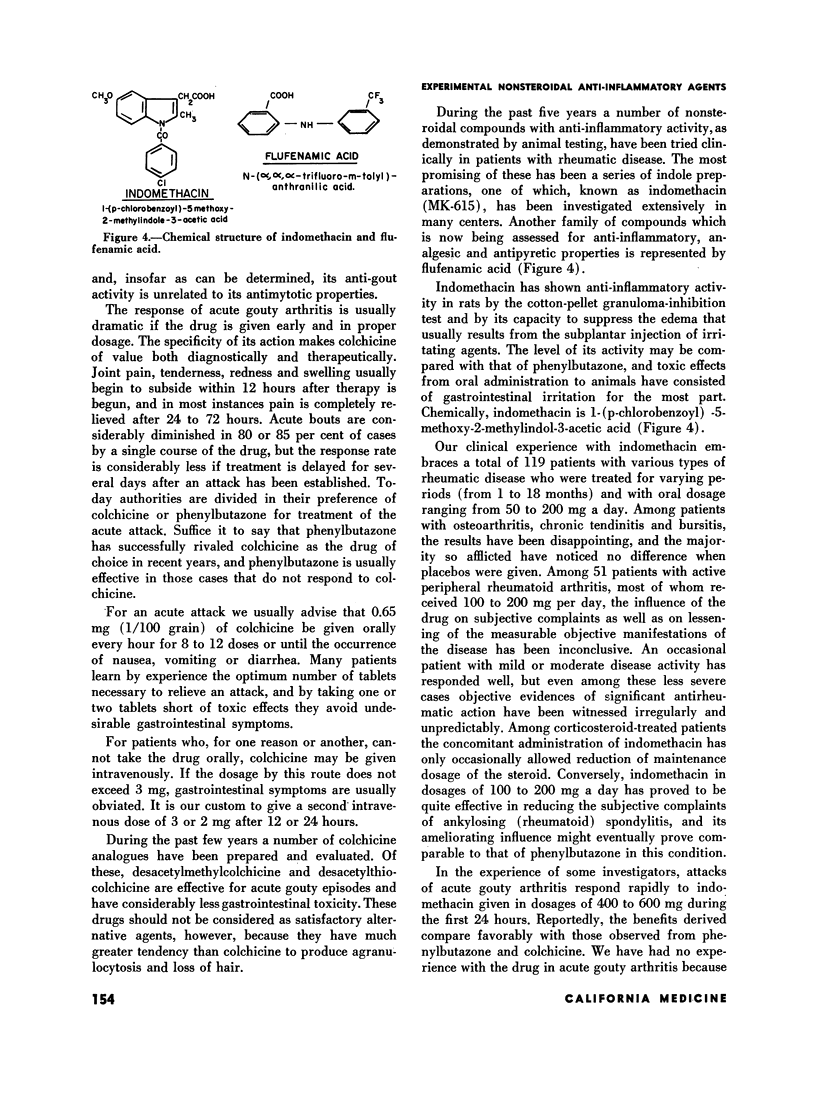
A number of indole preparations with anti-inflammatory activity have been tested clinically. One of them, indomethacin, has received extensive therapeutic trial; with dosages that can be tolerated the drug is fairly effective in the symptomatic control of ankylosing (rheumatoid) spondylitis but it is of questionable value in peripheral rheumatoid arthritis.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BOLAND E. W. Antirheumatic potency of chemically modified adrenocortical steroids. Am J Med. 1961 Oct;31:581–590. doi: 10.1016/0002-9343(61)90142-5. [DOI] [PubMed] [Google Scholar]
- BOLAND E. W. Clinical comparison of the newer anti-inflammatory corticosteroids. Ann Rheum Dis. 1962 Jun;21:176–187. doi: 10.1136/ard.21.2.176. [DOI] [PMC free article] [PubMed] [Google Scholar]