

Abstract
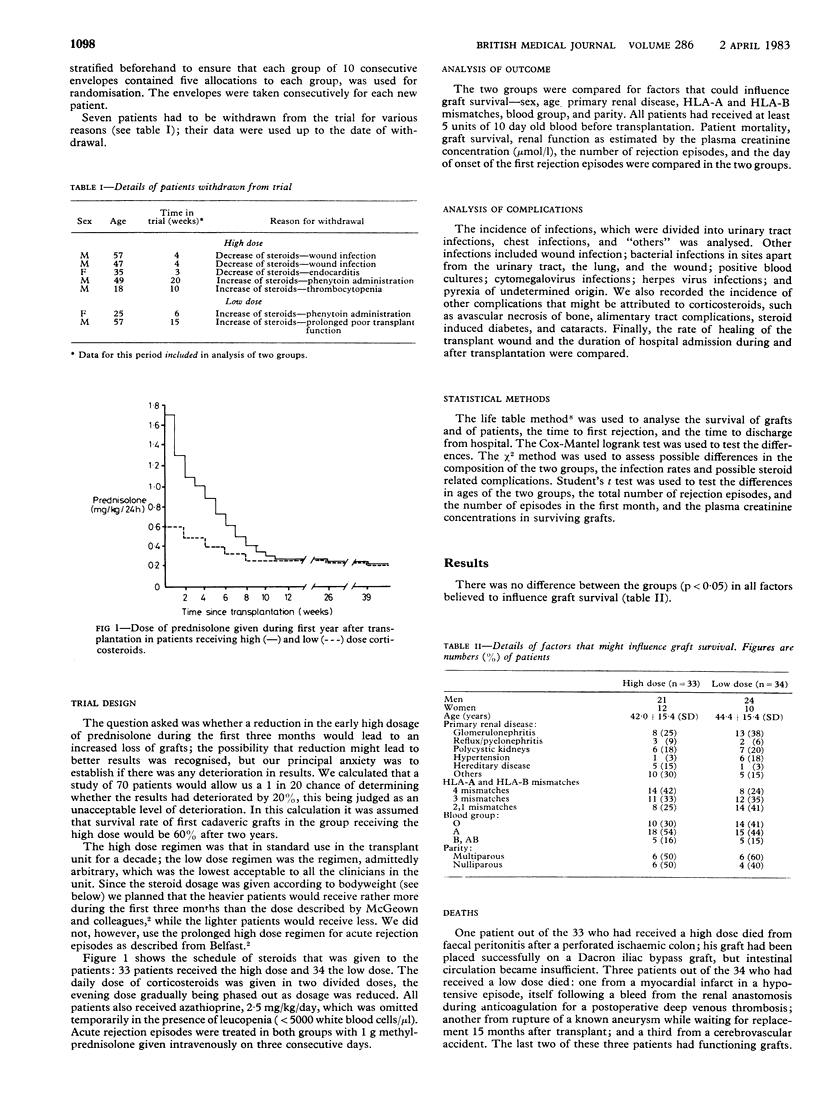
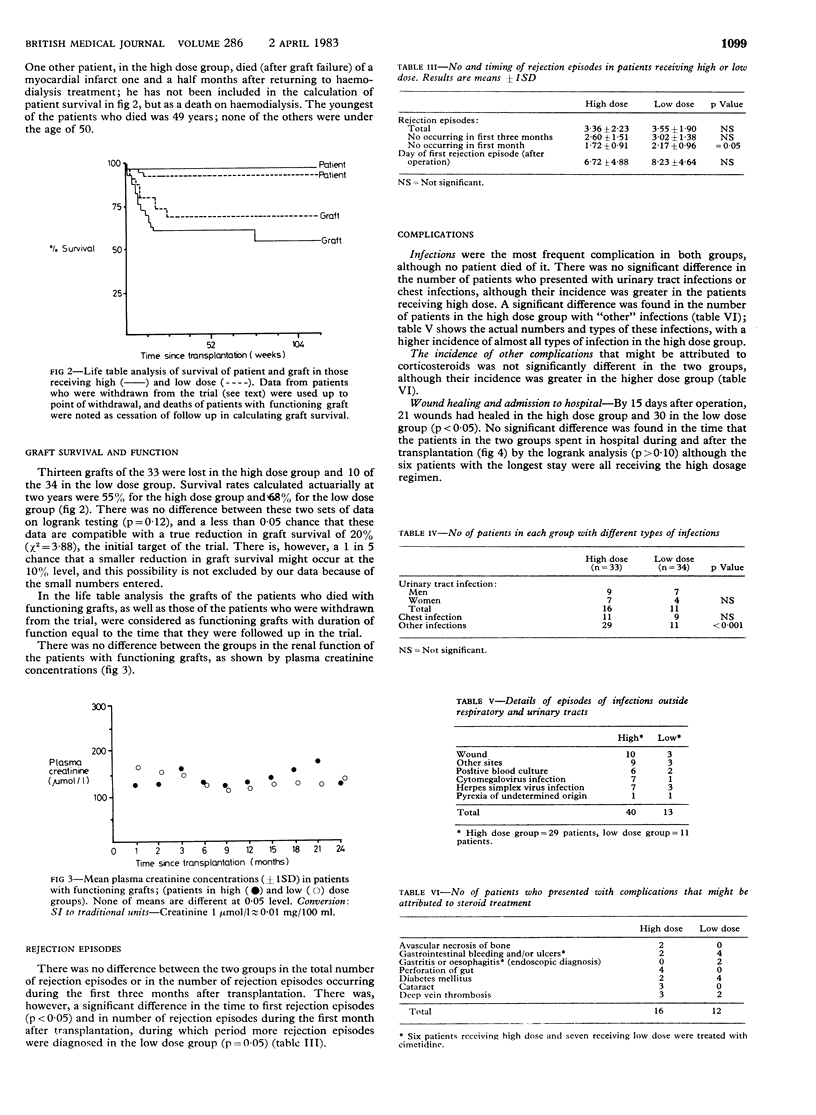
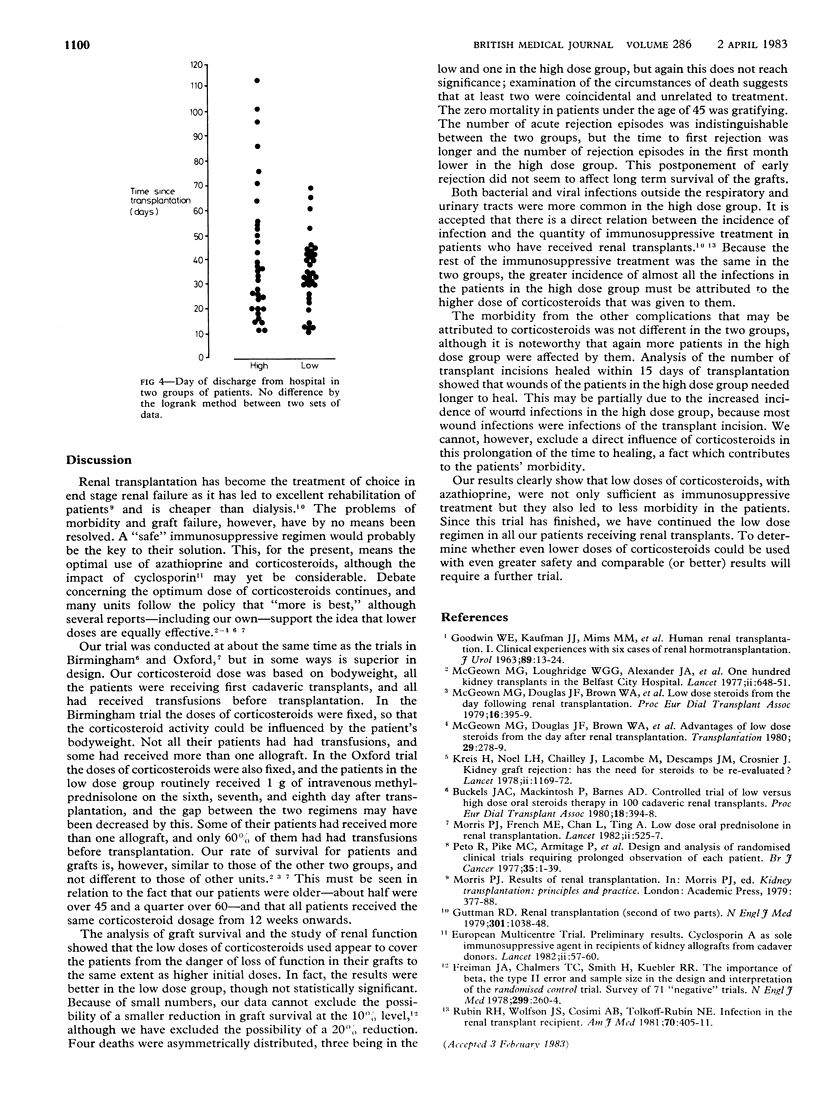
Corticosteroids have the major role in the immunosuppressive treatment of patients who have received renal transplants. Despite their extensive use there is still debate about the appropriate dose that will prevent rejection of the renal allograft with the least morbidity. From March 1979 to November 1981 a randomised controlled trial of high (33 patients) v low oral dose (34 patients) of prednisolone along with azathioprine was conducted in recipients of first cadaveric transplants who had received a blood transfusion within six months of transplantation. The main difference in outcome between the two groups was a high incidence of some infections in the high dose group. Patient mortality, graft survival, transplant function, and number of rejection episodes were indistinguishable in the two groups, but rejection episodes tended to occur later in the high dose group. These findings suggest that the use of lower doses of corticosteroids soon after cadaveric renal transplantation does not jeopardise graft survival and results in lower patient morbidity.
Full text
PDF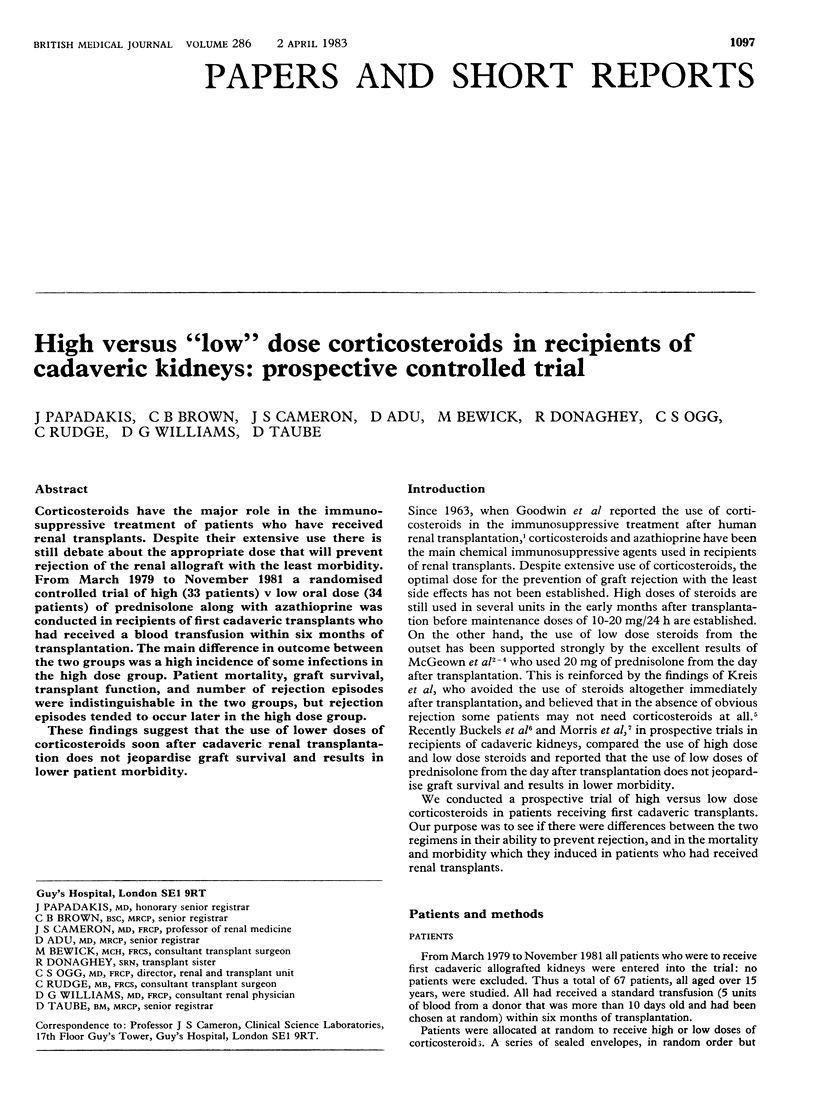
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Buckels J. A., Mackintosh P., Barnes A. D. Controlled trial of low versus high dose oral steroid therapy in 100 cadaveric renal transplants. Proc Eur Dial Transplant Assoc. 1981;18:394–399. [PubMed] [Google Scholar]
- GOODWIN W. E., KAUFMAN J. J., MIMS M. M., TURNER R. D., GLASSOCK R., GOLDMAN R., MAXWELL M. M. Human renal transplantation. I. Clinical experiences with six cases of renal homotransplantation. J Urol. 1963 Jan;89:13–24. doi: 10.1016/S0022-5347(17)64491-4. [DOI] [PubMed] [Google Scholar]
- Guttmann R. D. Renal transplantation (second of two parts). N Engl J Med. 1979 Nov 8;301(19):1038–1048. doi: 10.1056/NEJM197911083011905. [DOI] [PubMed] [Google Scholar]
- Kreis H., Lacombe M., Noel L. H., Descamps J. M., Chailley J., Crosnier J. Kidney-graft rejection: has the need for steroids to be re-evaluated? Lancet. 1978 Dec 2;2(8101):1169–1172. doi: 10.1016/s0140-6736(78)92153-0. [DOI] [PubMed] [Google Scholar]
- McGeown M. G., Douglas J. F., Brown W. A., Donaldson R. A., Kennedy J. A., Loughridge W. G., Mehta S., Hill C. M. Low dose steroid from the day following renal transplantation. Proc Eur Dial Transplant Assoc. 1979;16:395–400. [PubMed] [Google Scholar]
- McGeown M. G., Kennedy J. A., Loughridge W. G., Douglas J., Alexander J. A., Clarke S. D., McEvoy J., Hewitt J. C. One hundred kidney transplants in the Belfast city hospital. Lancet. 1977 Sep 24;2(8039):648–651. doi: 10.1016/s0140-6736(77)92512-0. [DOI] [PubMed] [Google Scholar]
- Morris P. J., Chan L., French M. E., Ting A. Low dose oral prednisolone in renal transplantation. Lancet. 1982 Mar 6;1(8271):525–527. doi: 10.1016/s0140-6736(82)92042-6. [DOI] [PubMed] [Google Scholar]
- Peto R., Pike M. C., Armitage P., Breslow N. E., Cox D. R., Howard S. V., Mantel N., McPherson K., Peto J., Smith P. G. Design and analysis of randomized clinical trials requiring prolonged observation of each patient. II. analysis and examples. Br J Cancer. 1977 Jan;35(1):1–39. doi: 10.1038/bjc.1977.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubin R. H., Wolfson J. S., Cosimi A. B., Tolkoff-Rubin N. E. Infection in the renal transplant recipient. Am J Med. 1981 Feb;70(2):405–411. doi: 10.1016/0002-9343(81)90780-4. [DOI] [PubMed] [Google Scholar]