

Abstract
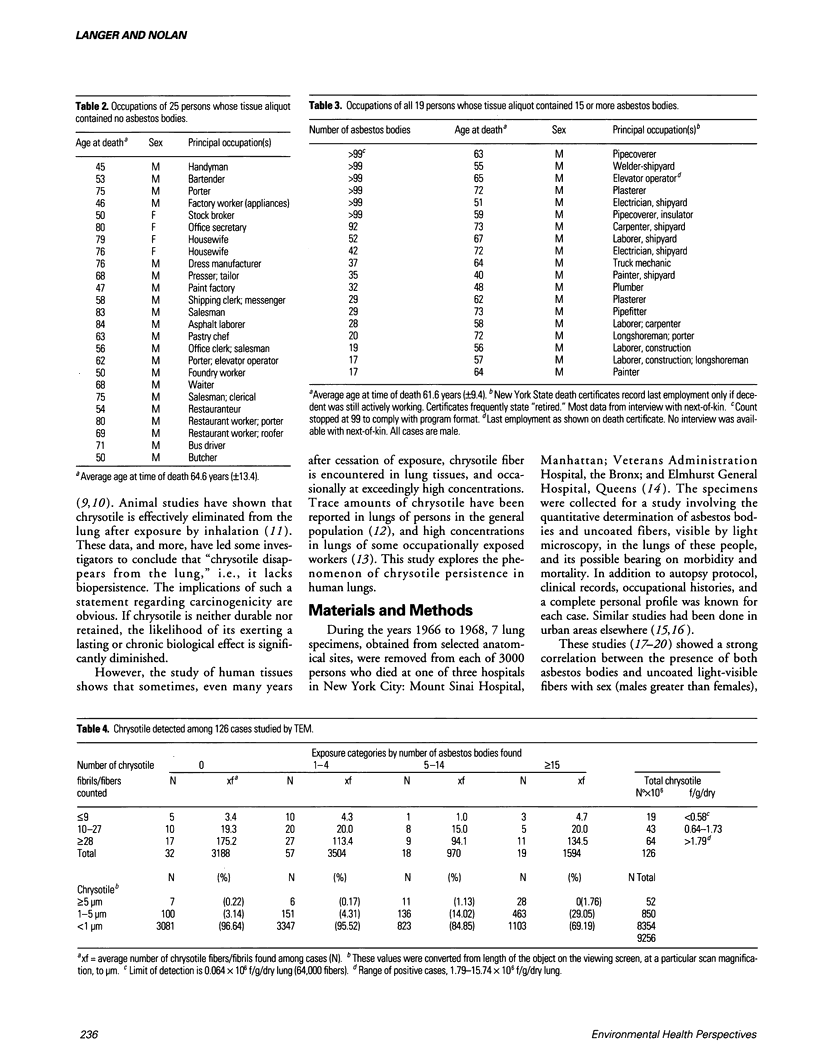
Lung burden analysis was performed on 126 autopsy cases of persons who died in New York City from 1966 through 1968. Of the 126 cases, 107 were probably non-occupationally exposed, judging by occupational history and asbestos body content of lung. Fifty-three of the 107 cases contained short chrysotile fibers/fibrils, < 5 microns in length, present in 3-fold greater amounts than were found in laboratory background controls. The fiber concentrations ranged from 1.8 to 15.7 x 10(6) f/gm/dry lung tissue, and the proportion of fibers > or = 5 microns in length was only 0.34% of the total chrysotile population found. Other inorganic particles present included fragments of amphiboles. In contrast to these data, the lung parenchyma of persons occupationally exposed to asbestos commonly showed the presence of other fiber types, especially amosite and crocidolite, at very much higher concentrations and greater fiber length. Any chrysotile present would usually be in fiber bundle form, with both fibers and fibrils > 5 microns in length. Comparison of the lung fiber content of occupationally exposed persons with that of the general population showed marked qualitative and quantitative differences. Fibers are durable, and are retained in a range of concentrations. Their length and dose, among other factors, which control their biological potential are different in the two populations; the risk factors for chrysotile-induced disease are not the same.
Full text
PDF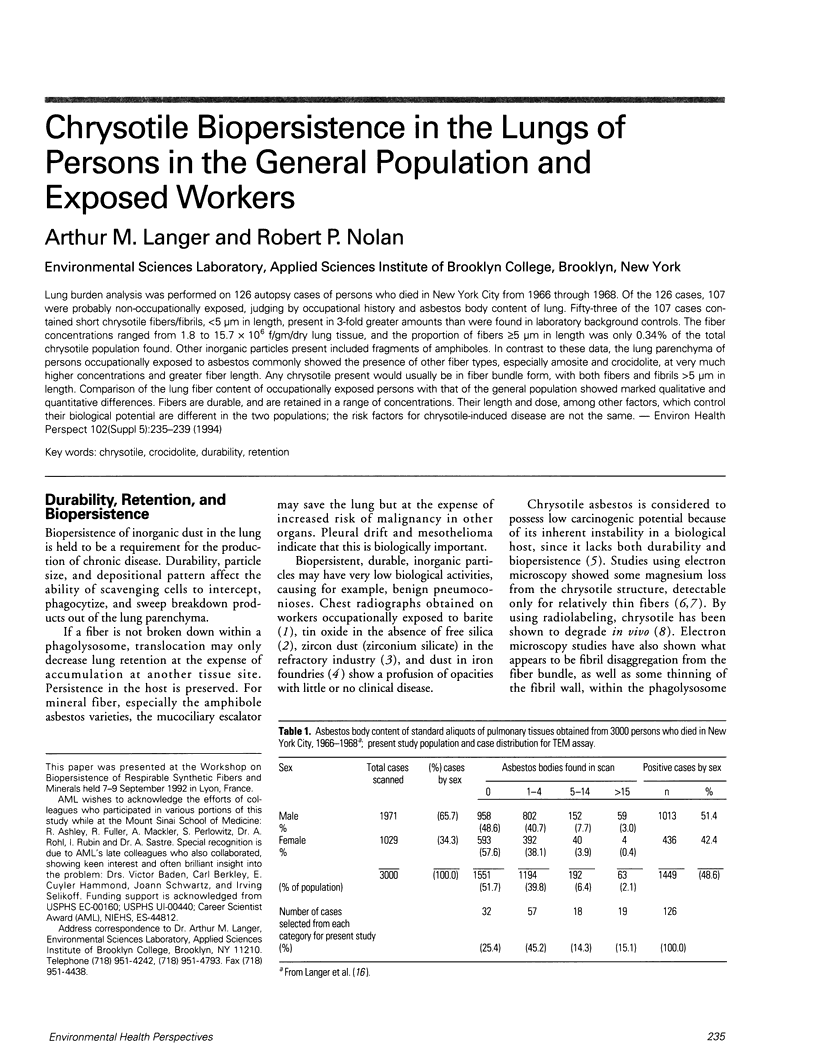

Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Langer A. M., Rubin I. B., Selikoff I. J., Pooley F. D. Chemical characterization of uncoated asbestos fibers from the lungs of asbestos workers by electron microprobe analysis. J Histochem Cytochem. 1972 Sep;20(9):735–740. doi: 10.1177/20.9.735. [DOI] [PubMed] [Google Scholar]
- Langer A. M., Selikoff I. J., Sastre A. Chrysotile asbestos in the lungs of persons in New York City. Arch Environ Health. 1971 Mar;22(3):348–361. doi: 10.1080/00039896.1971.10665854. [DOI] [PubMed] [Google Scholar]
- PANCHERI G. Su alcune forme di pneumoconiosi particolarmente studiate in Italia; tio-pneumoconiosi e baritosi. Med Lav. 1950 Mar;41(3):73–77. [PubMed] [Google Scholar]
- Suzuki Y., Churg J. Formation of the asbestos body. A comparative study with three types of asbestos. Environ Res. 1970 Mar;3(2):107–118. doi: 10.1016/0013-9351(70)90009-5. [DOI] [PubMed] [Google Scholar]
- Suzuki Y., Churg J. Structure and development of the asbestos body. Am J Pathol. 1969 Apr;55(1):79–107. [PMC free article] [PubMed] [Google Scholar]
- THOMSON J. G., KASCHULA R. O., MACDONALD R. R. Asbestos as a modern urban hazard. S Afr Med J. 1963 Jan 19;37:77–81. [PubMed] [Google Scholar]
- Thomson J. G. Asbestos and the urban dweller. Ann N Y Acad Sci. 1965 Dec 31;132(1):196–214. doi: 10.1111/j.1749-6632.1965.tb41102.x. [DOI] [PubMed] [Google Scholar]
- Wagner J. C., Berry G., Skidmore J. W., Timbrell V. The effects of the inhalation of asbestos in rats. Br J Cancer. 1974 Mar;29(3):252–269. doi: 10.1038/bjc.1974.65. [DOI] [PMC free article] [PubMed] [Google Scholar]