

Abstract
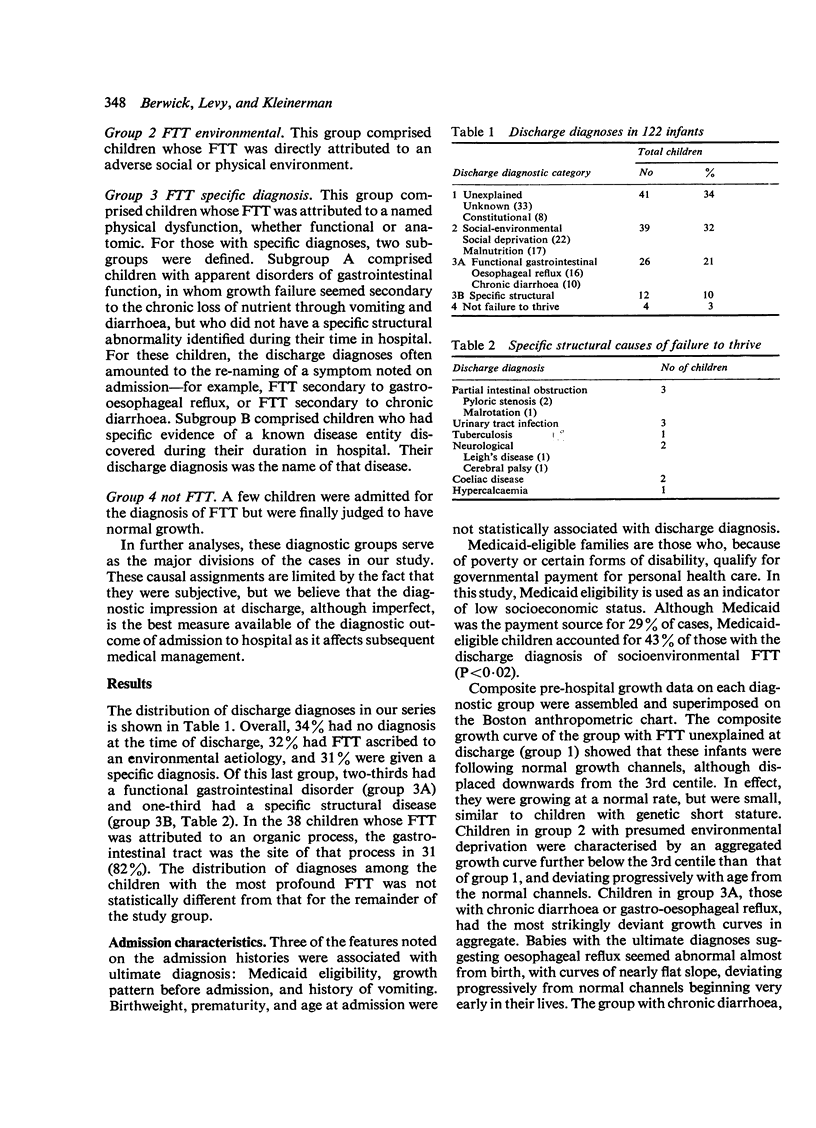
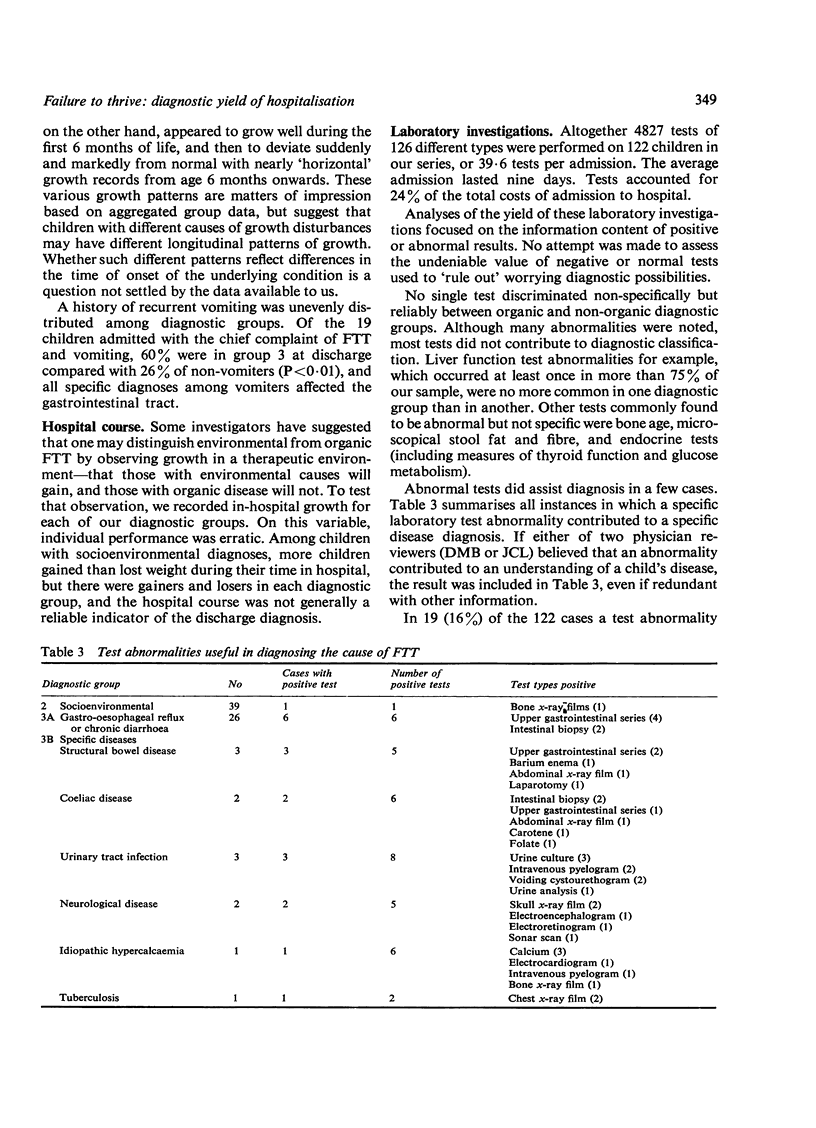
Review of hospital records of 122 infants, aged between 1 and 25 months, admitted to a teaching hospital with the diagnosis of failure to thrive but without an underlying disease apparent at admission, showed that about one-third of them had no diagnosis after evaluation. Thirty-two per cent were thought to have a social or environmental explantation for poor growth, and 31% were given a specific organic or physiological diagnosis. Of the last group, 2 out 3 were diagnosed as having either gastro-oesophageal reflux or non-specific chronic diarrhoea. Vomiting was often associated with organic or structural disease. On average about 40 laboratory tests and x-ray films were performed per infant, but only 0.8% of all tests showed an abnormality which contributed to the diagnosis of the cause of failure to thrive. Our results stress the importance of social and environmental factors as basic causes of failure to thrive, and suggest that admission to hospital and laboratory testing is unlikely to lead to a specific organic diagnose in a child whose failure to thrive is unexplained after careful history taking and a physical examination.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- AMBUEL J. P., HARRIS B. FAILURE TO THRIVE. A STUDY OF FAILURE TO GROW IN HEIGHT OR WEIGHT. Ohio State Med J. 1963 Oct;59:997–1001. [PubMed] [Google Scholar]
- Bullard D. M., Jr, Glaser H. H., Heagarty M. C., Pivchik E. C. Failure to thrive in the "neglected" child. Am J Orthopsychiatry. 1967 Jul;37(4):680–690. doi: 10.1111/j.1939-0025.1967.tb00509.x. [DOI] [PubMed] [Google Scholar]
- COLEMAN R. W., PROVENCE S. Environmental retardation (hospitalism) in infants living in families. Pediatrics. 1957 Feb;19(2):285–292. [PubMed] [Google Scholar]
- EISENBERG L., GLASER K. Maternal deprivation. Pediatrics. 1956 Oct;18(4):626–642. [PubMed] [Google Scholar]
- English P. C. Failure to thrive without organic reason. Pediatr Ann. 1978 Nov;7(11):774–781. [PubMed] [Google Scholar]
- Hannaway P. J. Failure to thrive: a study of 100 infants and children. Clin Pediatr (Phila) 1970 Feb;9(2):96–99. doi: 10.1177/000992287000900214. [DOI] [PubMed] [Google Scholar]
- Oates R. K., Yu J. S. Children with non-organic failure to thrive. A community problem. Med J Aust. 1971 Jul 24;2(4):199–203. [PubMed] [Google Scholar]
- Pollitt E. Failure to thrive: socioeconomic, dietary intake and mother-child interaction data. Fed Proc. 1975 Jun;34(7):1593–1597. [PubMed] [Google Scholar]
- Shaheen E., Alexander D., Truskowsky M., Barbero G. J. Failure to thrive--a retrospective profile. Clin Pediatr (Phila) 1968 May;7(5):255–261. doi: 10.1177/000992286800700505. [DOI] [PubMed] [Google Scholar]
- Sills R. H. Failure to thrive. The role of clinical and laboratory evaluation. Am J Dis Child. 1978 Oct;132(10):967–969. doi: 10.1001/archpedi.1978.02120350031003. [DOI] [PubMed] [Google Scholar]