

Abstract
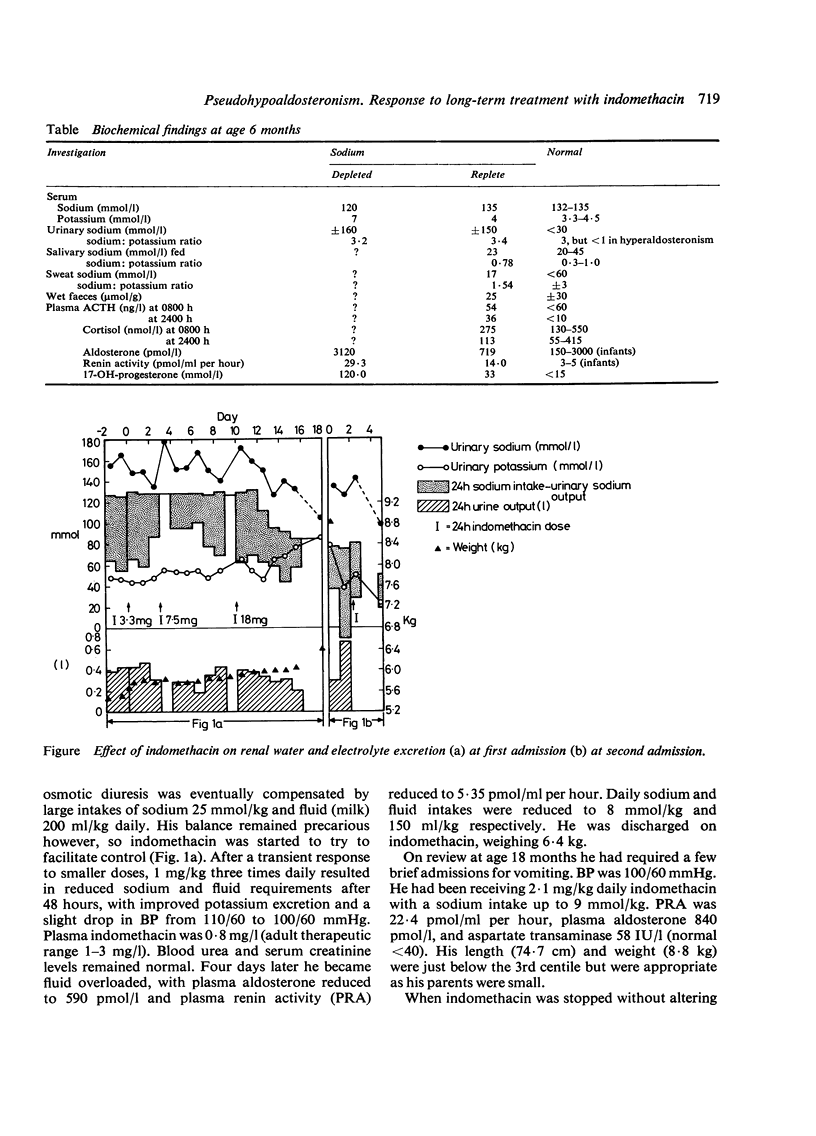
A 6-month-old boy presented with features of pseudohypoaldosteronism. Considerable quantities of supplemental sodium failed to compensate his natriuresis but indomethacin, a prostaglandin inhibitor, greatly reduced his sodium requirement. Treatment was maintained for 9 months when re-evaluation showed him to be dependent on indomethacin for satisfactory control.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bierich J. R., Schmidt U. Tubular Na, K-ATPase deficiency, the cause of the congenital renal salt-losing syndrome. Eur J Pediatr. 1976 Jan 2;121(2):81–87. doi: 10.1007/BF00443063. [DOI] [PubMed] [Google Scholar]
- Dillon M. J., Leonard J. V., Buckler J. M., Ogilvie D., Lillystone D., Honour J. W., Shackleton C. H. Pseudohypoaldosteronism. Arch Dis Child. 1980 Jun;55(6):427–434. doi: 10.1136/adc.55.6.427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee J. B., Patak R. V., Mookerjee B. K. Renal prostaglandins and the regulation of blood pressure and sodium and water homeostasis. Am J Med. 1976 May 31;60(6):798–816. doi: 10.1016/0002-9343(76)90893-7. [DOI] [PubMed] [Google Scholar]
- Oberfield S. E., Levine L. S., Carey R. M., Bejar R., New M. I. Pseudohypoaldosteronism: multiple target organ unresponsiveness to mineralocorticoid hormones. J Clin Endocrinol Metab. 1979 Feb;48(2):228–234. doi: 10.1210/jcem-48-2-228. [DOI] [PubMed] [Google Scholar]
- Rampini S., Furrer J., Keller H. P., Bucher H., Zachmann M. Congenital pseudohypoaldosteronism: case report and review. Effect of indomethacin during sodium chloride depletion. Helv Paediatr Acta. 1978 Jun;33(2):153–167. [PubMed] [Google Scholar]