

Abstract
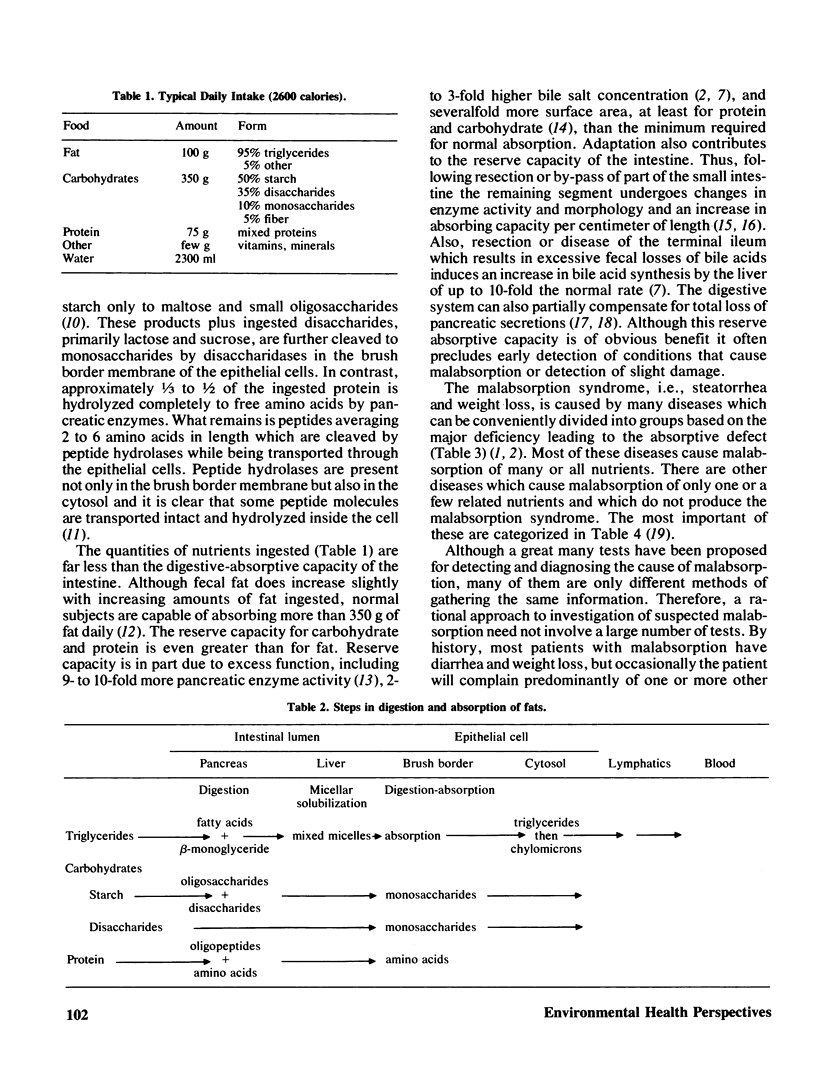
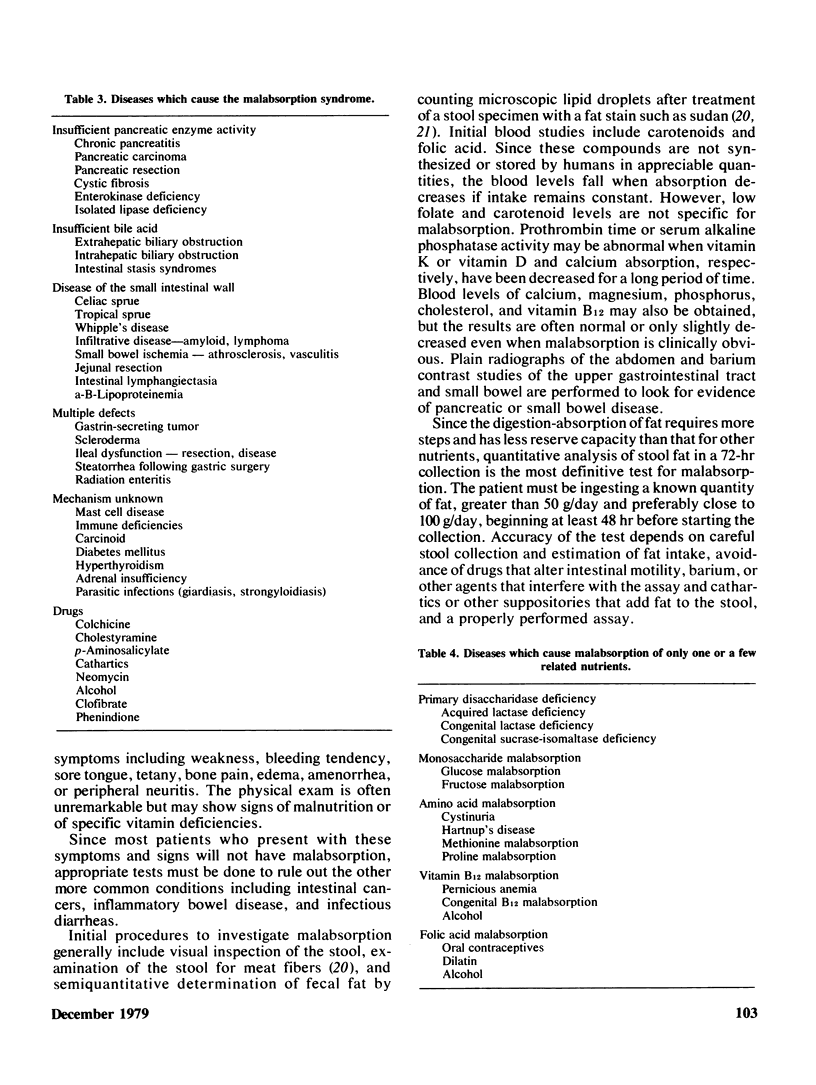
Adults eating a Western diet digest and absorb ingested food containing approximately 100 g fat, 350 g carbohydrate, and 75 g protein daily. Normal fat absorption requires adequate gastric, pancreatic, liver-biliary, mucosal, and lymphatic function. Carbohydrate and protein absorption is much less dependent on liver-biliary and lymphatic function. The intestine has a large reserve capacity for digestion and absorption of nutrients which is due to both excess function and to adaptive changes which increase function in one segment of the digestive-absorptive system when it is decreased or lost in another segment. The large reserve capacity explains why most of the prevalent intestinal diseases seldom cause clinically detectable changes in absorption. However, there are more than 30 less-common human diseases which cause malabsorption of one or more nutrients. Those that cause the malabsorption syndrome, i.e., steatorrhea and weight loss, can be conveniently categorized according to the major deficiency leading to the absorptive defect as follows: insufficient pancreatic enzyme activity, insufficient bile acid, disease of the small intestinal wall, multiple defects, mechanism unknown, and drug-induced malabsorption. A few diseases, most of which are congenital, cause malabsorption of only one or a few related nutrients such as lactose malabsorption in lactase deficiency. Most of the tests currently in use for detecting and diagnosing the cause of malabsorption are relatively insensitive and nonspecific. Chemical analysis of the fat in a three-day stool collection remains the single best test for diagnosing the malabsorption syndrome. However, a breath test using Triolein labeled with either the radioactive or stable isotope of carbon may be an important recent advance. Other breath tests are also currently being investigated for quantitating absorption or malabsorption of various substances including bile acids and various sugars. Studies of the function of the intestinal epithelial cells are usually best accomplished using tissue obtained by per oral biopsy. Biopsy specimens are used for many types of study including light and electron microscopic examination, chemical and enzymatic assays, tissue culture, and uptake of various radiolabeled compounds.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BENSON J. A., Jr, CULVER P. J., RAGLAND S., JONES C. M., DRUMMEY G. D., BOUGAS E. The d-xylose absorption test in malabsorption syndromes. N Engl J Med. 1957 Feb 21;256(8):335–339. doi: 10.1056/NEJM195702212560802. [DOI] [PubMed] [Google Scholar]
- Beck I. T. The role of pancreatic enzymes in digestion. Am J Clin Nutr. 1973 Mar;26(3):311–325. doi: 10.1093/ajcn/26.3.311. [DOI] [PubMed] [Google Scholar]
- Bond J. H., Jr, Levitt M. D., Prentiss R. Investigation of small bowel transit time in man utilizing pulmonary hydrogen (H2) measurements. J Lab Clin Med. 1975 Apr;85(4):546–555. [PubMed] [Google Scholar]
- Borgström B. On the interactions between pancreatic lipase and colipase and the substrate, and the importance of bile salts. J Lipid Res. 1975 Nov;16(6):411–417. [PubMed] [Google Scholar]
- Brindley D. N. The intracellular phase of fat absorption. Biomembranes. 1974;4B(0):621–671. doi: 10.1007/978-1-4684-3336-4_2. [DOI] [PubMed] [Google Scholar]
- Curtis K. J., Gaines H. D., Kim Y. S. Protein digestion and absorption in rats with pancreatic duct occlusion. Gastroenterology. 1978 Jun;74(6):1271–1276. [PubMed] [Google Scholar]
- DRUMMEY G. D., BENSON J. A., Jr, JONES C. M. Microscopical examination of the stool for steatorrhea. N Engl J Med. 1961 Jan 12;264:85–87. doi: 10.1056/NEJM196101122640207. [DOI] [PubMed] [Google Scholar]
- DiMagno E. P., Go V. L., Summerskill W. H. Relations between pancreatic enzyme outputs and malabsorption in severe pancreatic insufficiency. N Engl J Med. 1973 Apr 19;288(16):813–815. doi: 10.1056/NEJM197304192881603. [DOI] [PubMed] [Google Scholar]
- FINLAY J. M., HOGARTH J., WIGHTMAN K. J. A CLINICAL EVALUATION OF THE D-XYLOSE TOLERANCE TEST. Ann Intern Med. 1964 Sep;61:411–422. doi: 10.7326/0003-4819-61-3-411. [DOI] [PubMed] [Google Scholar]
- FLICK A. L., QUINTON W. E., RUBIN C. E. A peroral hydraulic biopsy tube for multiple sampling at any level of the gastro-intestinal tract. Gastroenterology. 1961 Jan;40:120–126. [PubMed] [Google Scholar]
- Hofmann A. F., Lauterburg B. H. Breath test with isotopes of carbon: progress and potential. J Lab Clin Med. 1977 Sep;90(3):405–411. [PubMed] [Google Scholar]
- Krawitt E. L., Beeken W. L. Limitations of the usefulness of the d-xylose absorption test. Am J Clin Pathol. 1975 Feb;63(2):261–263. doi: 10.1093/ajcp/63.2.261. [DOI] [PubMed] [Google Scholar]
- Lauterburg B. H., Newcomer A. D., Hofmann A. F. Clinical value of the bile acid breath test. Evaluation of the Mayo Clinic experience. Mayo Clin Proc. 1978 Apr;53(4):227–233. [PubMed] [Google Scholar]
- Matthews D. M. Intestinal absorption of peptides. Physiol Rev. 1975 Oct;55(4):537–608. doi: 10.1152/physrev.1975.55.4.537. [DOI] [PubMed] [Google Scholar]
- Milne M. D. Hereditary disorders of intestinal transport. Biomembranes. 1974;4B(0):961–1013. doi: 10.1007/978-1-4684-3336-4_9. [DOI] [PubMed] [Google Scholar]
- Moore J. G., Englert E., Jr, Bigler A. H., Clark R. W. Simple fecal tests of absorption. A prospective study and critique. Am J Dig Dis. 1971 Feb;16(2):97–105. doi: 10.1007/BF02284442. [DOI] [PubMed] [Google Scholar]
- Newcomer A. D., McGill D. B., Thomas P. J., Hofmann A. F. Prospective comparison of indirect methods for detecting lactase deficiency. N Engl J Med. 1975 Dec 11;293(24):1232–1236. doi: 10.1056/NEJM197512112932405. [DOI] [PubMed] [Google Scholar]
- Perera D. R., Weinstein W. M., Rubin C. E. Symposium on pathology of the gastrointestinal tract-Part II. Small intestinal biopsy. Hum Pathol. 1975 Mar;6(2):157–217. doi: 10.1016/s0046-8177(75)80176-6. [DOI] [PubMed] [Google Scholar]
- Schoeller D. A., Schneider J. F., Solomons N. W., Watkins J. B., Klein P. D. Clinical diagnosis with the stable isotope 13C in CO2 breath tests: methodology and fundamental considerations. J Lab Clin Med. 1977 Sep;90(3):412–421. [PubMed] [Google Scholar]
- Waldmann T. A. Protein-losing enteropathy. Gastroenterology. 1966 Mar;50(3):422–443. [PubMed] [Google Scholar]
- Watkins J. B., Schoeller D. A., Klein P. D., Ott D. G., Newcomer A. D., Hofmann A. F. 13C-trioctanoin: a nonradioactive breath test to detect fat malabsorption. J Lab Clin Med. 1977 Sep;90(3):422–430. [PubMed] [Google Scholar]
- Williamson R. C. Intestinal adaptation (first of two parts). Structural, functional and cytokinetic changes. N Engl J Med. 1978 Jun 22;298(25):1393–1402. doi: 10.1056/NEJM197806222982505. [DOI] [PubMed] [Google Scholar]
- Wollaeger E. E. Role of the ileum in fat absorption. Mayo Clin Proc. 1973 Dec;48(12):836–843. [PubMed] [Google Scholar]