

Abstract
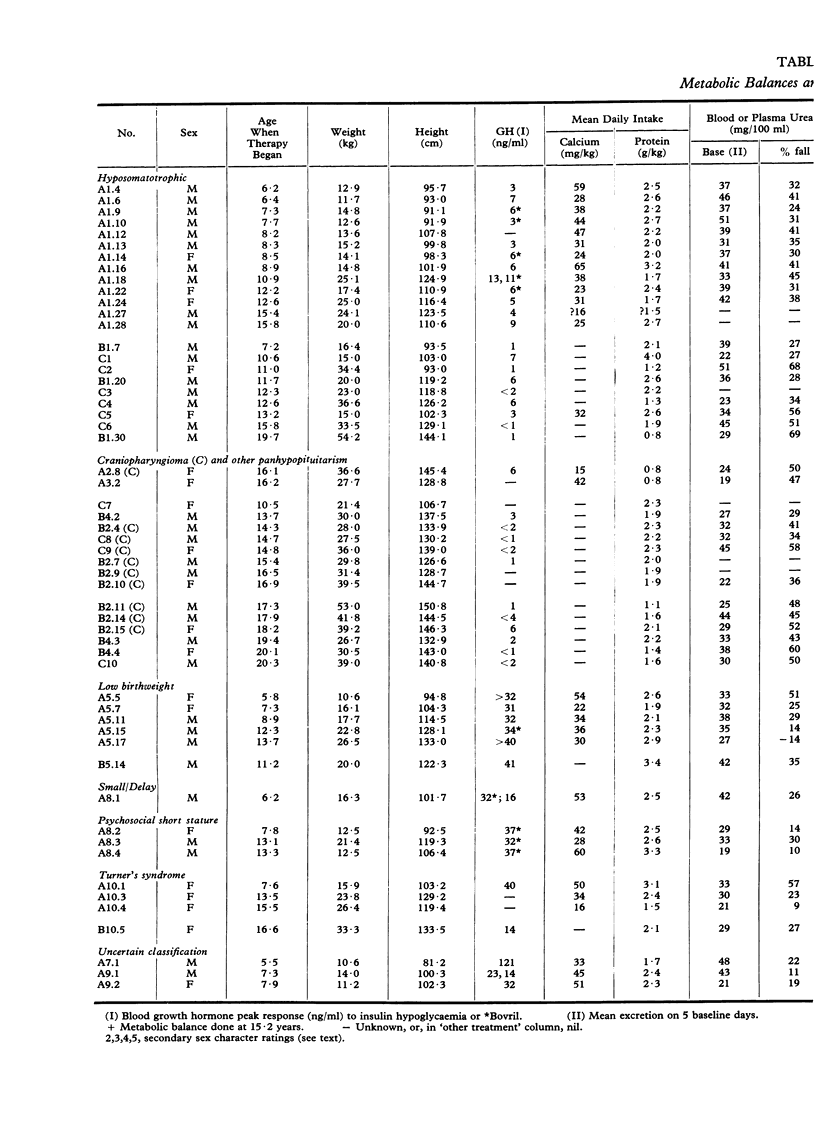
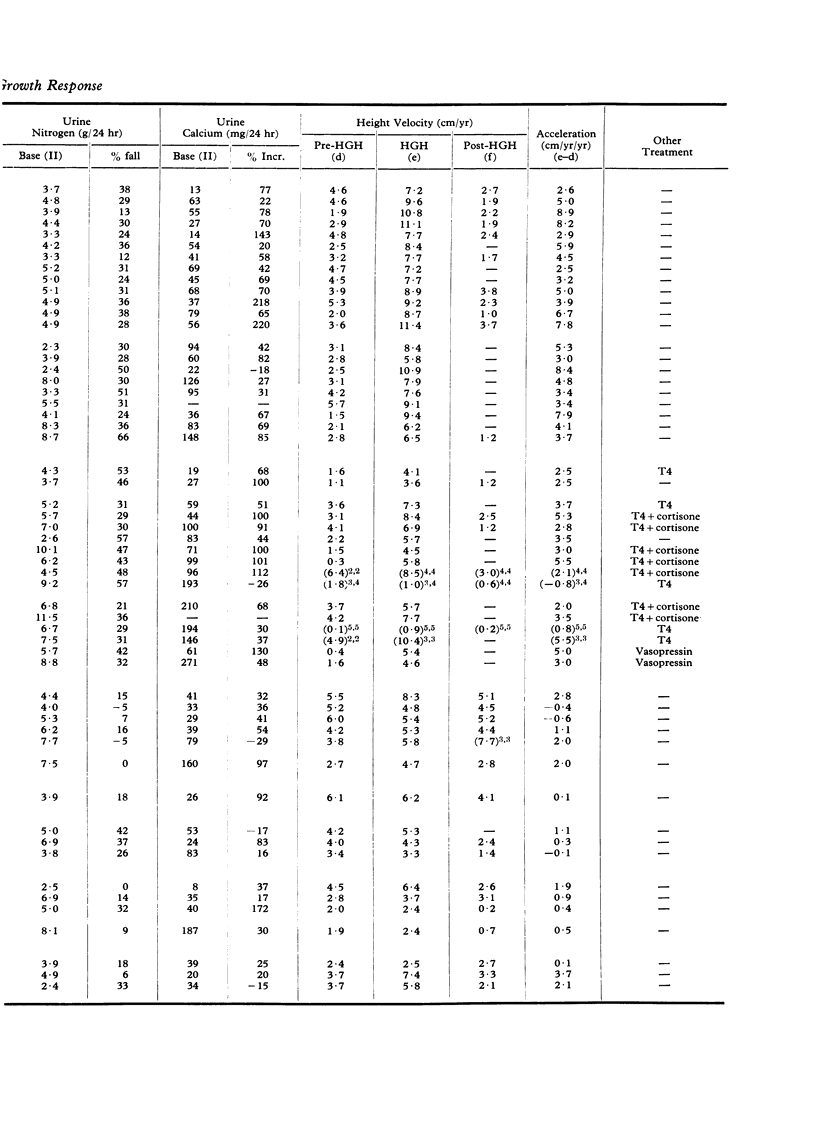
Metabolic tests of the response to three days of administration of human growth hormone (HGH) have been done on 55 patients aged 6·2 to 20·3 years. 22 had `isolated' growth hormone deficiency (or hyposomatotrophic short stature, HS), 16 CNS tumours or multiple hormone deficiencies, 6 short stature associated with low birthweight, 3 psychosocial short stature, 4 Turner's syndrome, 1 hereditary short stature, and 3 uncertain diagnosis. Height was measured at 3-monthly intervals for a full year, then HGH was given for a full year and the difference in rate, that is the acceleration during the growth hormone year, was calculated. The height measurements were all done by one measurer in 45 of the patients.
In the metabolic test there were 5 baseline days followed by 3 days of a single injection of 10 IU HGH, then 2 final days. The means for urinary nitrogen excretion, blood urea, and urinary calcium excretion were calculated for the 5 baseline days and for the last 2 HGH days plus the one subsequent day. The difference between the means is given as a percentage of baseline values.
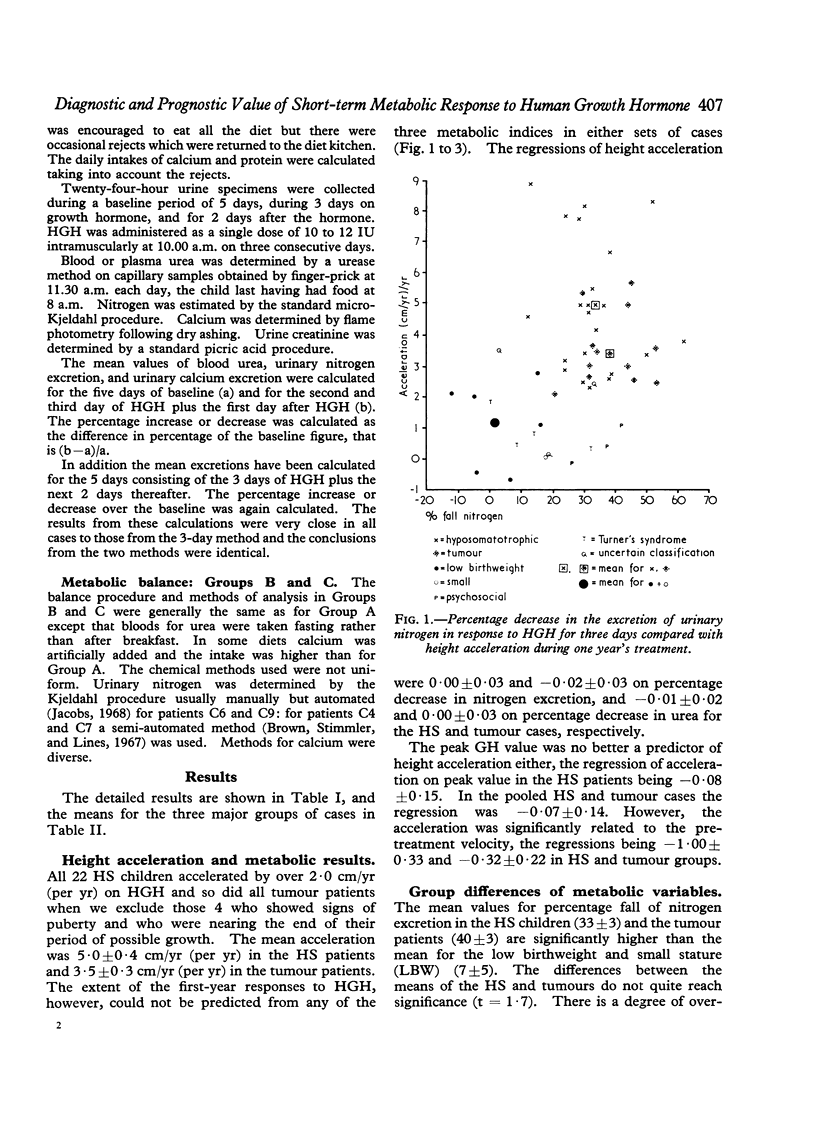
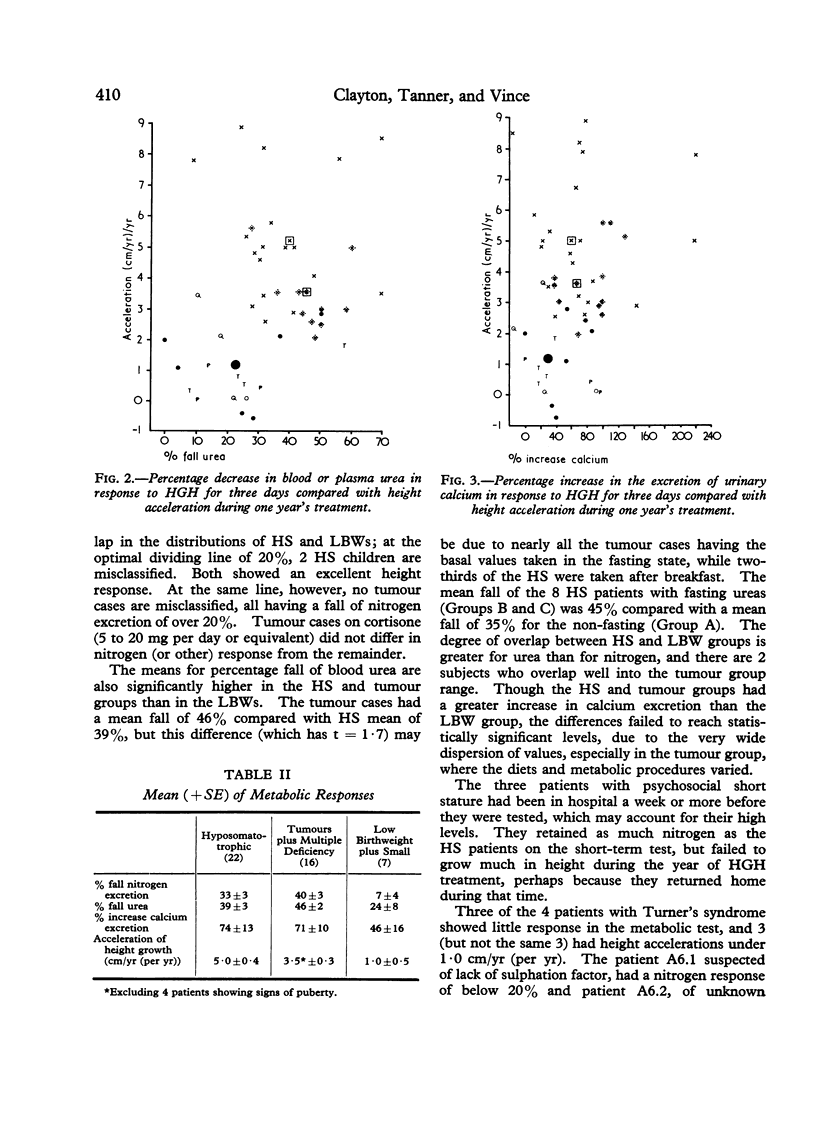
The children with isolated growth hormone (GH) deficiency had a greater decrease in nitrogen excretion (33±3%) than the low birthweight cases and small children (7±5%), but there was overlap between individuals in the isolated deficiency group (range 12 to 66%) and the rest (range -12% to 42%); 2 deficient children were below a dividing line of 20%, and 1 Turner's syndrome and 3 psychosocial short stature children were above it. The tumour and multiple deficiency patients had an average fall of 40±3% and showed no overlap with the low birthweight group. Blood urea and calcium excretion gave a worse separation. Within the isolated deficiency and the tumour and multiple deficiency groups there was no relation between any metabolic parameter and the amount of growth acceleration in the first year of HGH treatment.
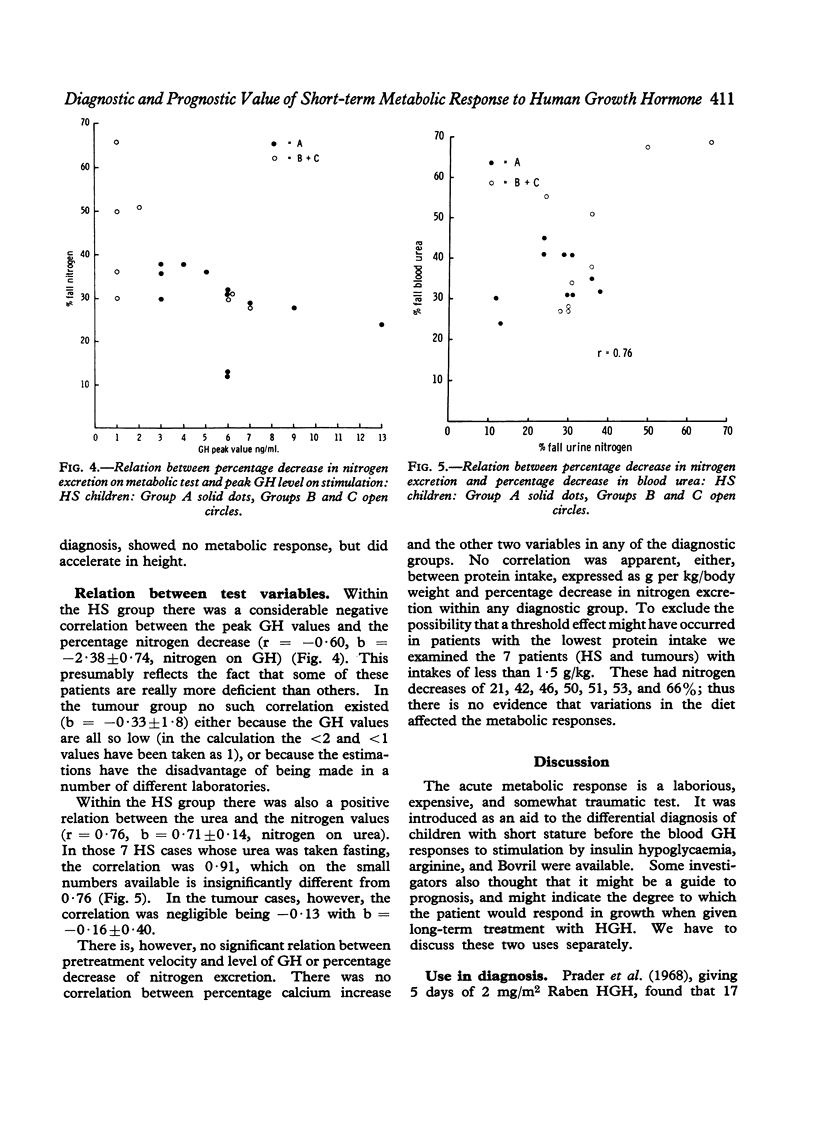
In the HS, though not in the tumour patients, there was a correlation (-0·60) between the decrease in percentage nitrogen excretion and peak GH level on stimulation and between per cent decrease in urinary nitrogen excretion and per cent decrease in blood urea (0·76).
We conclude that the differential diagnostic value of the short-term metabolic test is very limited now that we have tests of GH response; and that in cases of isolated GH or multiple pituitary hormone deficiency the result of the metabolic test does not predict at all the height acceleration obtained on HGH treatment.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BECK J. C., McGARRY E. E., DYRENFURTH I., VENNING E. H. The metabolic effects of human and monkey growth hormone in man. Ann Intern Med. 1958 Nov;49(5):1090–1105. doi: 10.7326/0003-4819-49-5-1090. [DOI] [PubMed] [Google Scholar]
- Brown G. A., Stimmler L., Lines J. G. Growth hormone-induced nitrogen retention in children of short stature. Arch Dis Child. 1967 Jun;42(223):239–244. doi: 10.1136/adc.42.223.239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chalkley S. R., Tanner J. M. Incidence and effects on growth of antibodies to human growth hormone. Arch Dis Child. 1971 Apr;46(246):160–166. doi: 10.1136/adc.46.246.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- HENNEMAN P. H., FORBES A. P., MOLDAWER M., DEMPSEY E. F., CARROLL E. L. Effects of human growth hormone in man. J Clin Invest. 1960 Aug;39:1223–1238. doi: 10.1172/JCI104138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacobs S. C. Assessment of automated nitrogen analysis of biological fluids with reference to the Kjeldahl method. J Clin Pathol. 1968 Mar;21(2):218–219. doi: 10.1136/jcp.21.2.218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Melvin K. E., Wright A. D., Hartog M., Antcliff A. C., Copestake A. M., Fraser T. R. Acute metabolic response to human growth hormone in different types of dwarfism. Br Med J. 1967 Jul 22;3(5559):196–199. doi: 10.1136/bmj.3.5559.196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PRADER A., ILLIG R., SZEKY J., WAGNER H. THE EFFECT OF HUMAN GROWTH HORMONE IN HYPOPITUITARY DWARFISM. Arch Dis Child. 1964 Dec;39:535–544. doi: 10.1136/adc.39.208.535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prader A., Zachmann M., Poley J. R., Illig R., Széky J. Long-term treatment with human growth hormone (Raben) in small doses. Evaluation of 18 hypopituitary patients. Helv Paediatr Acta. 1967 Oct;22(5):423–440. [PubMed] [Google Scholar]
- Prader A., Zachmann M., Poley J. R., Illig R. The metabolic effect of a small uniform dose of human growth hormone in hypopituitary dwarfs and in control children. I. Nitrogen, alpha-amino-N, creatine-creatinine and calcium excretion and serum urea-N, alpha-amino-N, inorganic phosphorus and alkaline phosphatase. Acta Endocrinol (Copenh) 1968 Jan;57(1):115–128. doi: 10.1530/acta.0.0570115. [DOI] [PubMed] [Google Scholar]
- WRIGHT J. C., BRASEL J. A., ACETO T., Jr, FINKELSTEIN J. W., KENNY F. M., SPAULDING J. S., BLIZZARD R. M. STUDIES WITH HUMAN GROWTH HORMONE (HGH). Am J Med. 1965 Apr;38:499–516. doi: 10.1016/0002-9343(65)90128-2. [DOI] [PubMed] [Google Scholar]
- Youlton R., Kaplan S. L., Grumbach M. M. Growth and growth hormone. IV. Limitations of the growth hormone response to insulin and arginine and of the immunoreactive insulin response to arginine in the assessment of growth hormone deficiency in children. Pediatrics. 1969 Jun;43(6):989–1004. [PubMed] [Google Scholar]