

Abstract
Newborn infants with suspected bacterial infection were treated with intramuscular gentamicin. Serum levels of the drug were measured 1 hour after the first dose, immediately before the second dose, and immediately before and 1 hour after a dose given on the third day.
On a low dosage regimen (1 mg/kg every 8 hours) 9 of 17 infants had serum gentamicin levels below the required minimum level of 1 μg/ml immediately before the second dose, and 5 of 19 infants had similarly low levels on the third day. On a high dosage regimen (3 mg/kg initially, then 2 mg/kg every 8 hours) 2 of 10 infants had preinjection serum gentamicin levels below 1 μg/ml on the first day, and 3 out of 16 had similar levels on the third day. The mean (± SE) serum gentamicin level on the high dosage regimen was 5·0 ± 0·5 μg/ml 1 hour after the first injection, 1·9 ± 0·4 μg/ml just before the second injection, and on the third day 1·9 ± 0·3 μg/ml just before an injection and 5·1 ± 0·5 μg/ml 1 hour after injection. The highest serum gentamicin level recorded in any of the 40 infants studied was 8·2 μg/ml.
On the first day of treatment with the low dose regimen, a mean of 21% (range 9-68%) of the injected dose was recovered from the urine; and on the third or fourth day a mean of 44% (range 17-76%) of the gentamicin injected on that day was recovered.
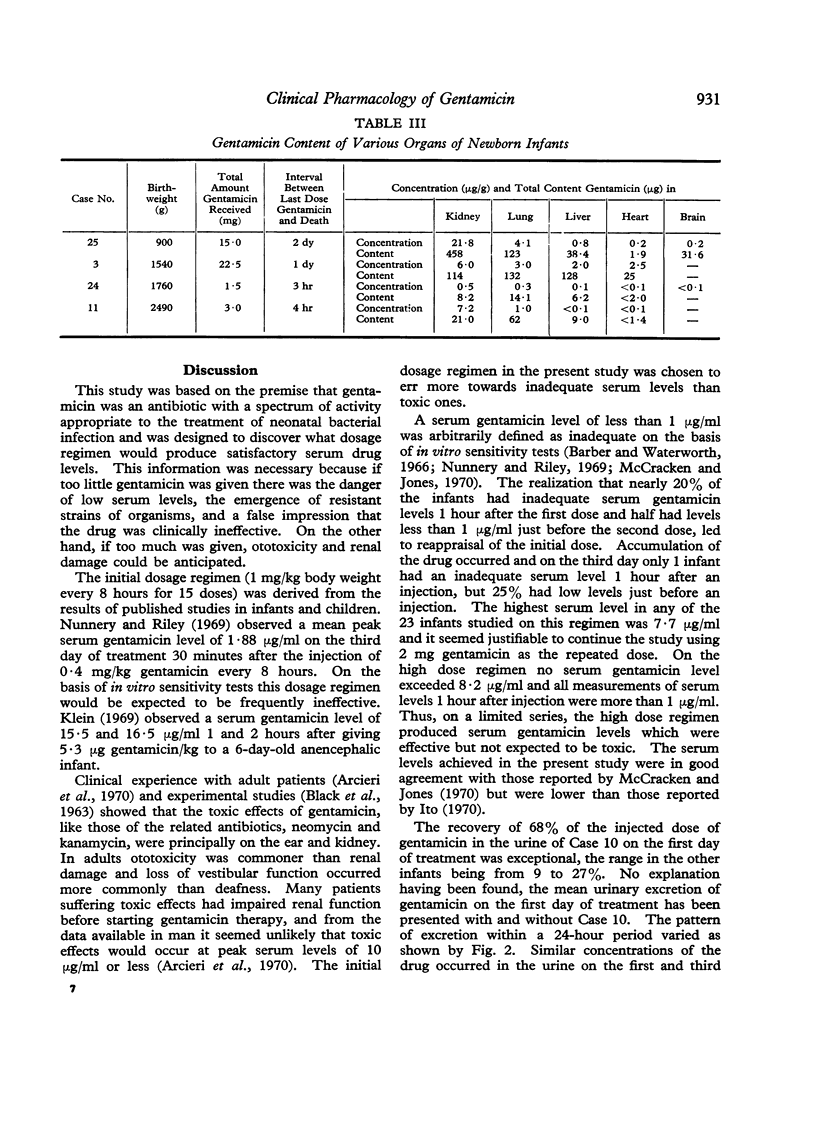
In 4 infants who died tissue gentamicin levels were measured in the liver, lungs, heart, kidneys, and brain, the highest concentration being in the kidney with low levels in the heart, liver, and brain, while levels in the lungs were intermediate. Neonatal renal and pulmonary infections are thus likely to be suitably treated with gentamicin.
Bacteriological studies confirmed the effectiveness of gentamicin in the treatment of neonatal infection, but a dosage regimen derived by extrapolation from older children frequently resulted in inadequate serum levels, and a higher dosage regimen giving more satisfactory results was therefore defined.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BLACK J., CALESNICK B., WILLIAMS D., WEINSTEIN M. J. PHARMACOLOGY OF GENTAMICIN, A NEW BROAD-SPECTRUM ANTIBIOTIC. Antimicrob Agents Chemother (Bethesda) 1963;161:138–147. [PubMed] [Google Scholar]
- Barber M., Waterworth P. M. Activity of gentamicin against Pseudomonas and hospital Staphylococci. Br Med J. 1966 Jan 22;1(5481):203–205. doi: 10.1136/bmj.1.5481.203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ito T. [Absorption, excretion and effects of gentamicin in newborn infants]. Jpn J Antibiot. 1970 Jun;23(3):298–311. [PubMed] [Google Scholar]
- Klein J. O. Consideration of gentamicin for therapy of neonatal sepsis. J Infect Dis. 1969 Apr-May;119(4):457–459. doi: 10.1093/infdis/119.4-5.457. [DOI] [PubMed] [Google Scholar]
- McCracken G. H., Jr, Jones L. G. Gentamicin in the neonatal period. Am J Dis Child. 1970 Dec;120(6):524–533. doi: 10.1001/archpedi.1970.02100110072007. [DOI] [PubMed] [Google Scholar]
- Nunnery A. W., Riley H. D., Jr Gentamicin: pharmacologic observations in newborns and infants. J Infect Dis. 1969 Apr-May;119(4):402–405. doi: 10.1093/infdis/119.4-5.402. [DOI] [PubMed] [Google Scholar]