

Abstract
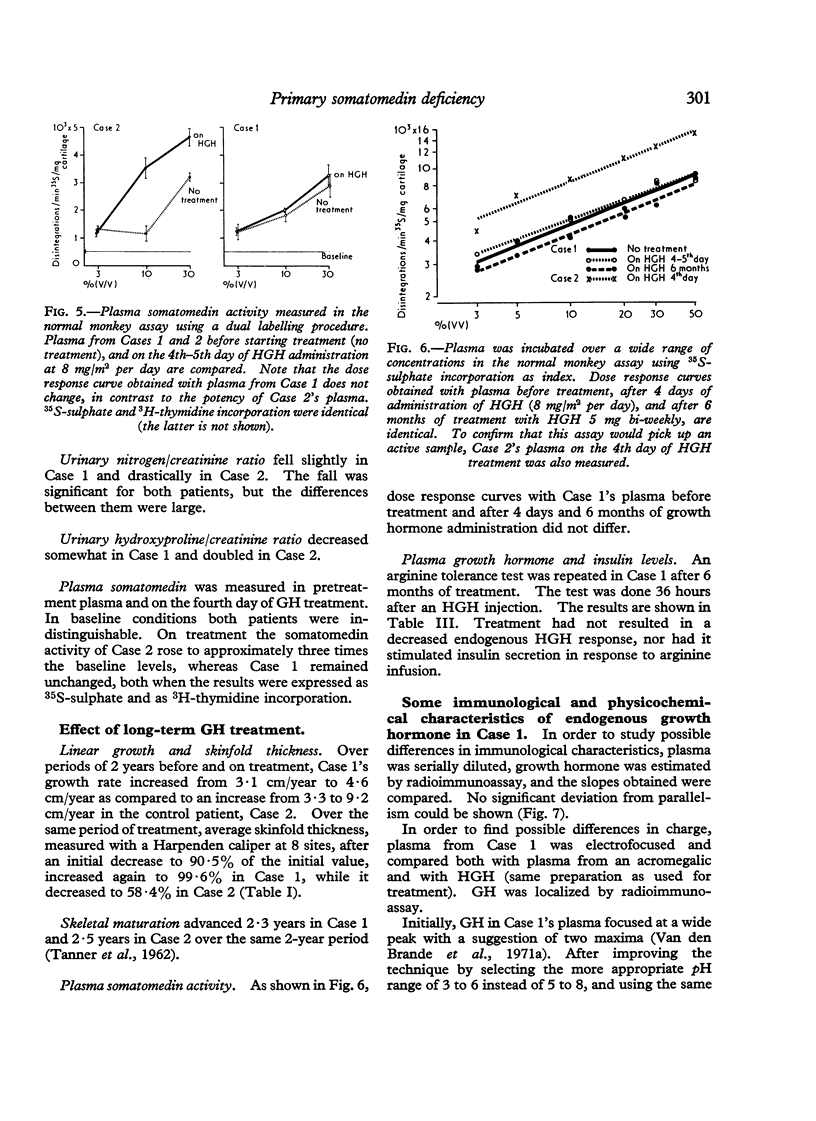
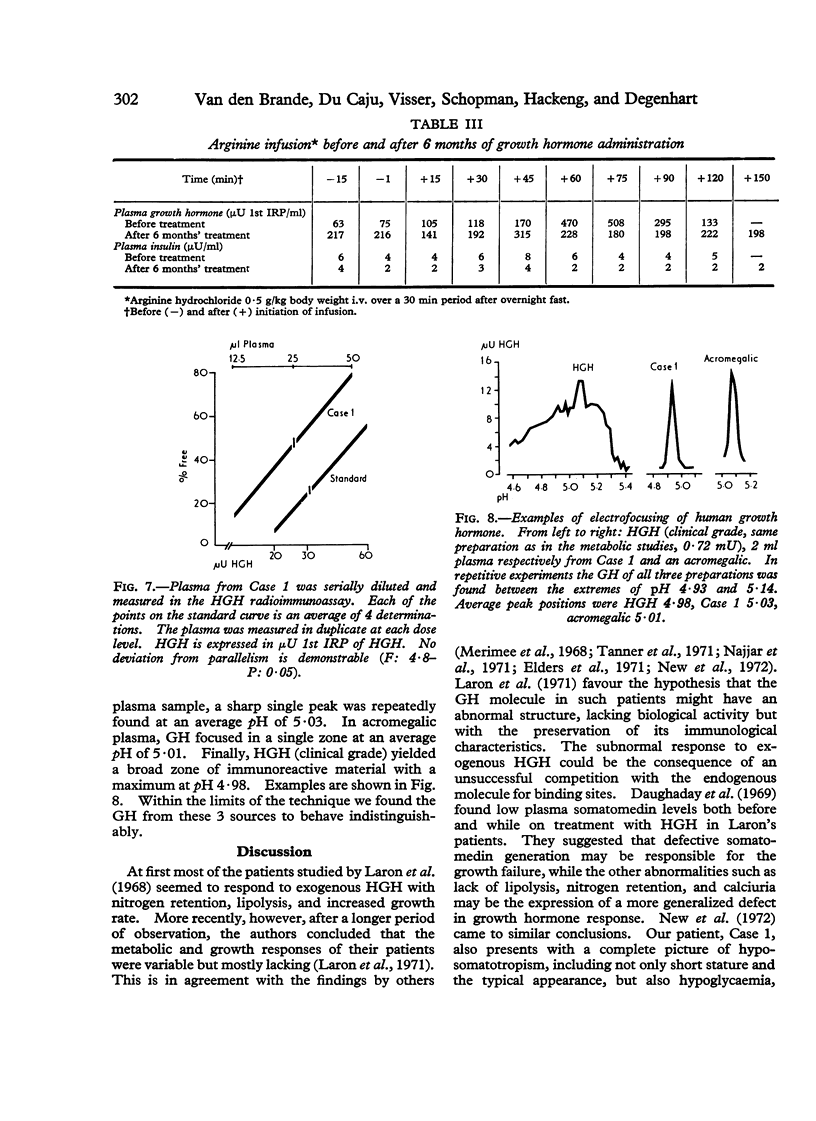
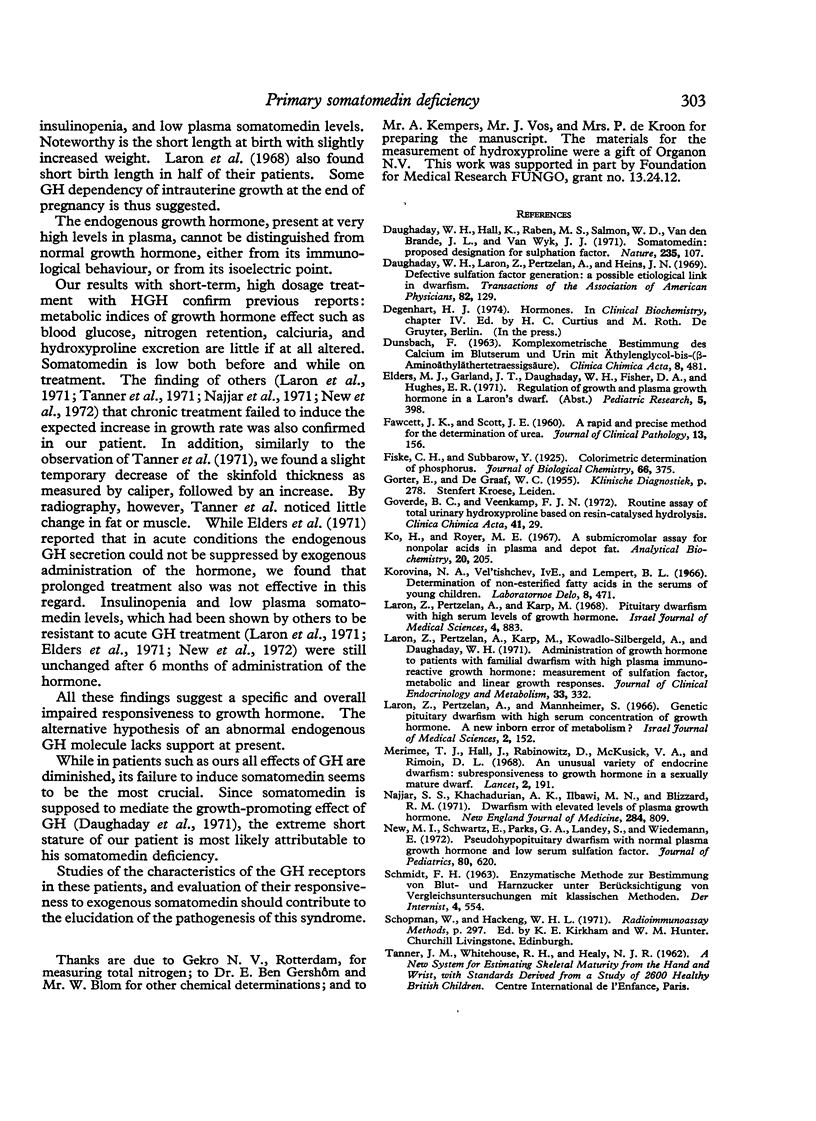
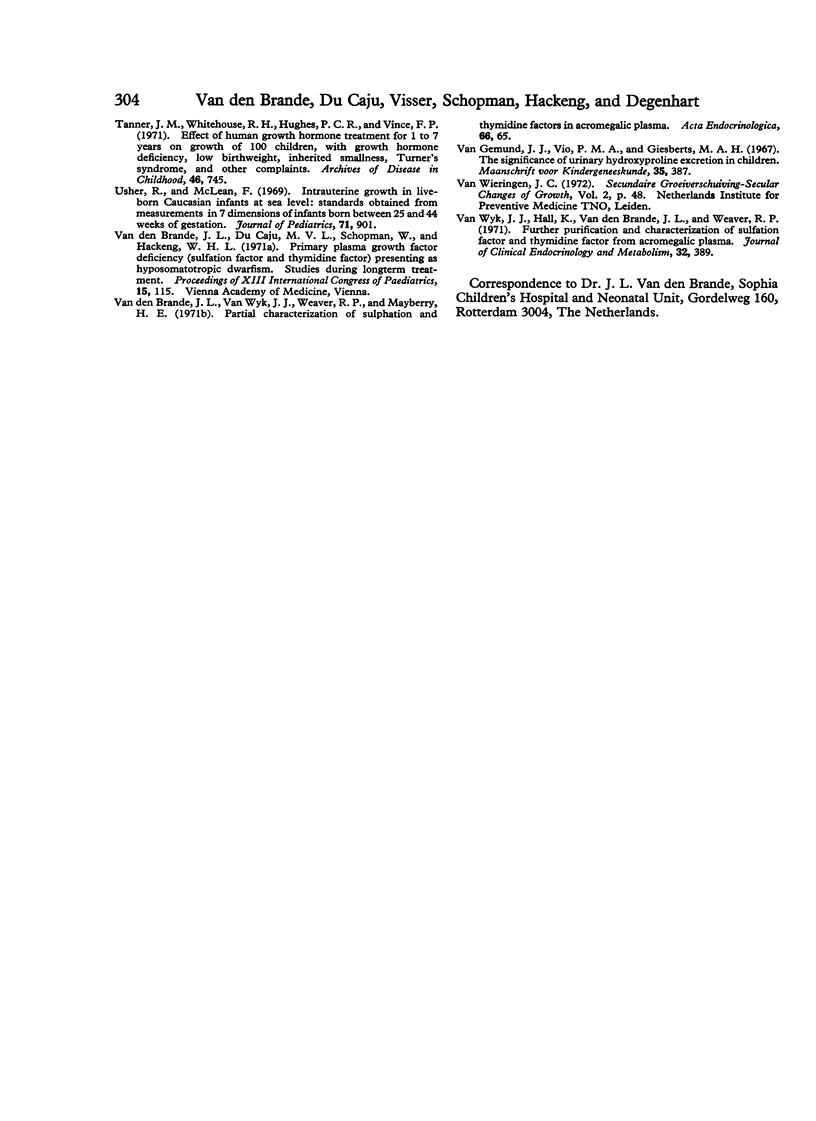
A child presenting with the clinical features of hyposomatotropism but with high immunoreactive plasma growth hormone is described. During short-term administration of human growth hormone (HGH) his response with regard to fasting blood-glucose and free fatty acids, plasma-somatomedin, urinary excretion of calcium, nitrogen, and hydroxyproline was minimal or absent. 6 months of treatment with HGH did not reduce the endogenous HGH secretion. Insulin secretion had not increased and plasma somatomedin levels remained extremely low. Over a period of 2 years of treatment, growth response and loss of subcutaneous fat were minimal. On serial dilution in radioimmunoassay, his growth hormone (GH) molecule yielded a parallel line with the HGH standard. In electrofocusing experiments the GH molecule was in the same pH range as growth hormone in acromegalic plasma and the major peak of clinical grade HGH (5·03 against 5·01 and 4·98).
It is concluded that an overall and specific diminished responsiveness to HGH is present in this patient. This includes a lack of generation of somatomedin, which is thought to be the cause of his short stature. There was no evidence of abnormality of the GH molecule.
Full text
PDF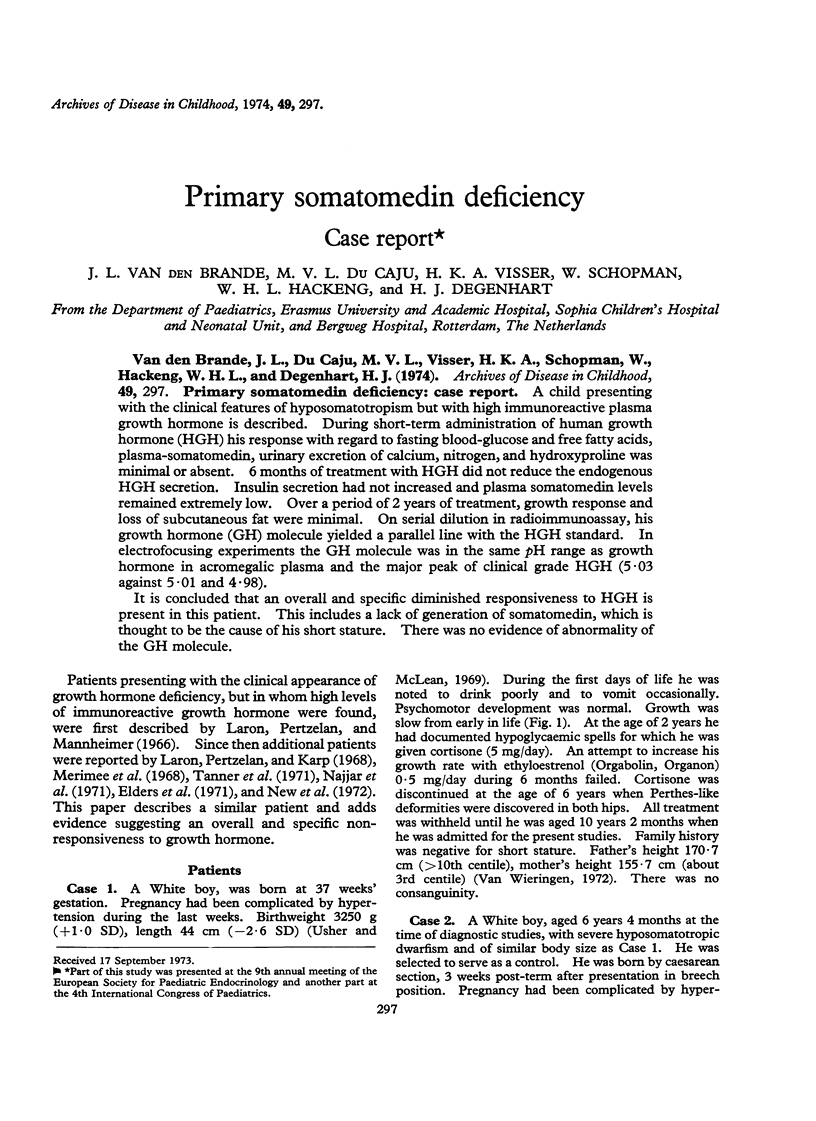
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Daughaday W. H., Hall K., Raben M. S., Salmon W. D., Jr, van den Brande J. L., van Wyk J. J. Somatomedin: proposed designation for sulphation factor. Nature. 1972 Jan 14;235(5333):107–107. doi: 10.1038/235107a0. [DOI] [PubMed] [Google Scholar]
- Daughaday W. H., Laron Z., Pertzelan A., Heins J. N. Defective sulfation factor generation: a possible etiological link in dwarfism. Trans Assoc Am Physicians. 1969;82:129–140. [PubMed] [Google Scholar]
- FAWCETT J. K., SCOTT J. E. A rapid and precise method for the determination of urea. J Clin Pathol. 1960 Mar;13:156–159. doi: 10.1136/jcp.13.2.156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goverde B. C., Veenkamp F. J. Routine assay of total urinary hydroxyproline based on resin-catalysed hydrolysis. Clin Chim Acta. 1972 Oct;41:29–40. doi: 10.1016/0009-8981(72)90492-5. [DOI] [PubMed] [Google Scholar]
- Ko H., Royer M. E. A submicromolar assay for nonpolar acids in plasma and depot fat. Anal Biochem. 1967 Aug;20(2):205–214. doi: 10.1016/0003-2697(67)90026-7. [DOI] [PubMed] [Google Scholar]
- Laron Z., Pertzelan A., Karp M., Kowadlo-Silbergeld A., Daughaday W. H. Administration of growth hormone to patients with familial dwarfism with high plasma immunoreactive growth hormone: measurement of sulfation factor, metabolic and linear growth responses. J Clin Endocrinol Metab. 1971 Aug;33(2):332–342. doi: 10.1210/jcem-33-2-332. [DOI] [PubMed] [Google Scholar]
- Laron Z., Pertzelan A., Karp M. Pituitary dwarfism with high serum levels of growth hormone. Isr J Med Sci. 1968 Jul-Aug;4(4):883–894. [PubMed] [Google Scholar]
- Laron Z., Pertzelan A., Mannheimer S. Genetic pituitary dwarfism with high serum concentation of growth hormone--a new inborn error of metabolism? Isr J Med Sci. 1966 Mar-Apr;2(2):152–155. [PubMed] [Google Scholar]
- Merimee T. J., Hall J., Rabinowitz D., McKusick V. A., Rimoin D. L. An unusual variety of endocrine dwarfism: subresponsiveness to growth hormone in a sexually mature dwarf. Lancet. 1968 Jul 27;2(7561):191–193. doi: 10.1016/s0140-6736(68)92623-8. [DOI] [PubMed] [Google Scholar]
- Najjar S. S., Khachadurian A. K., Ilbawi M. N., Blizzard R. M. Dwarfism with elevated levels of plasma growth hormone. N Engl J Med. 1971 Apr 15;284(15):809–812. doi: 10.1056/NEJM197104152841502. [DOI] [PubMed] [Google Scholar]
- New M. I., Schwartz E., Parks G. A., Landey S., Wiedemann E. Pseudohypopituitary dwarfism with normal plasma growth hormone and low serum sulfation factor. J Pediatr. 1972 Apr;80(4):620–626. doi: 10.1016/s0022-3476(72)80059-3. [DOI] [PubMed] [Google Scholar]
- SCHMIDT F. H. ENZYMATISCHE METHODEN ZUR BESTIMMUNG VON BLUT- UND HARNZUCKER UNTER BERUECKSICHTIGUNG VON VERGLEICHSUNTERSUCHUNGEN MIT KLASSISCHEN METHODEN. Internist (Berl) 1963 Dec;4:554–559. [PubMed] [Google Scholar]
- Tanner J. M., Whitehouse R. H., Hughes P. C., Vince F. P. Effect of human growth hormone treatment for 1 to 7 years on growth of 100 children, with growth hormone deficiency, low birthweight, inherited smallness, Turner's syndrome, and other complaints. Arch Dis Child. 1971 Dec;46(250):745–782. doi: 10.1136/adc.46.250.745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Usher R., McLean F. Intrauterine growth of live-born Caucasian infants at sea level: standards obtained from measurements in 7 dimensions of infants born between 25 and 44 weeks of gestation. J Pediatr. 1969 Jun;74(6):901–910. doi: 10.1016/s0022-3476(69)80224-6. [DOI] [PubMed] [Google Scholar]
- Van Wyk J. J., Hall K., Van den Brande J. L., Weaver R. P. Further purification and characterization of sulfation factor and thymidine factor from acromegalic plasma. J Clin Endocrinol Metab. 1971 Mar;32(3):389–403. doi: 10.1210/jcem-32-3-389. [DOI] [PubMed] [Google Scholar]
- Van den Brande J. L., Van Wyk J. J., Weaver R. P., Mayberry H. E. Partial characterization of sulphation and thymidine factors in acromegalic plasma. Acta Endocrinol (Copenh) 1971 Jan;66(1):65–81. doi: 10.1530/acta.0.0660065. [DOI] [PubMed] [Google Scholar]