

Abstract
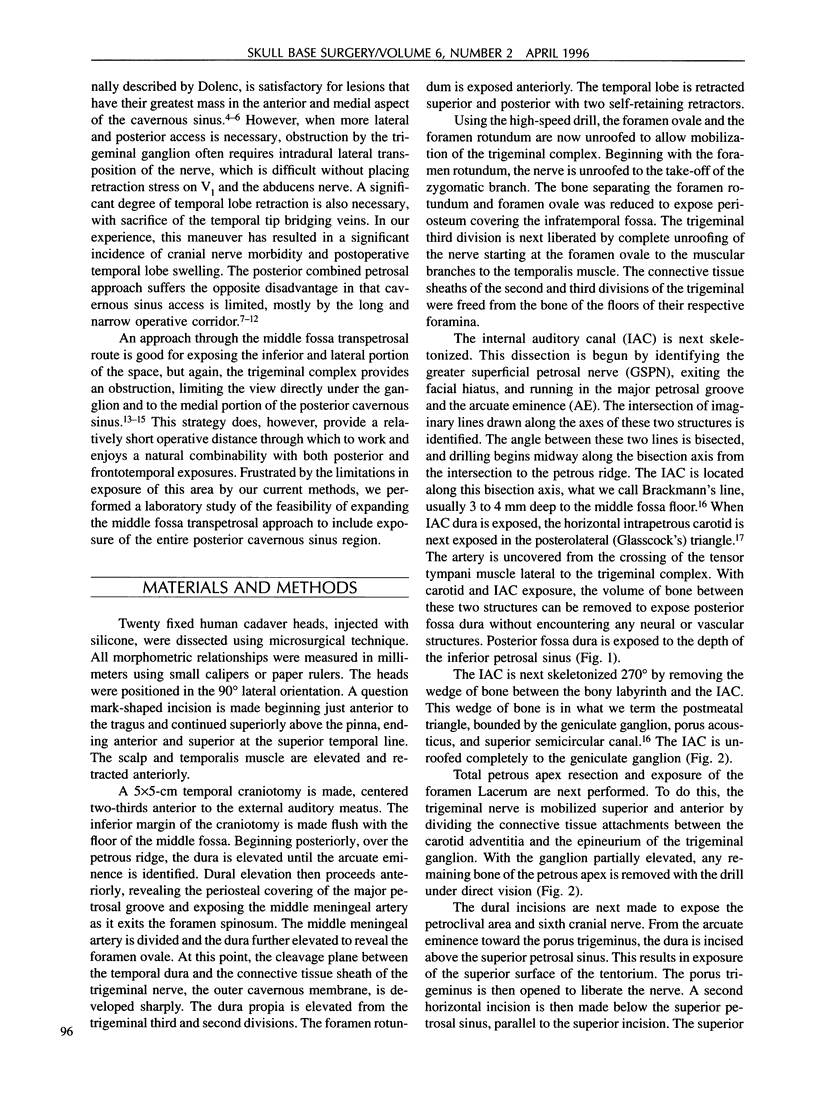
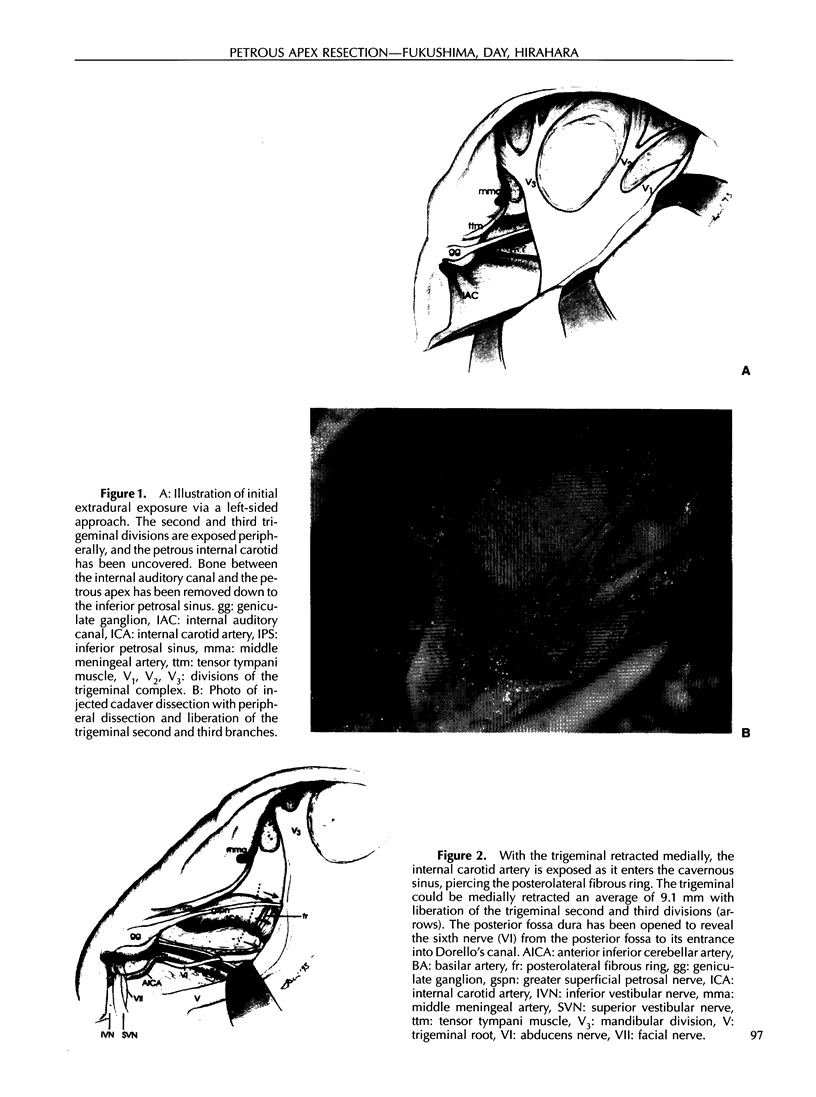
We have analyzed a strategy for improved exposure of the posterior cavernous sinus and petroclival region through an extradural subtemporal approach to be utilized in the removal of neoplastic processes with involvement of the apical petrous bone and posterior cavernous sinus. This surgical approach includes the following elements for improved exposure of the posterior cavernous sinus through the middle fossa corridor: (1) maximal extradural exposure and mobilization of the trigeminal nerve complex, allowing its elevation and anterior displacement, (2) complete extradural removal of the anterior petrous pyramid from the porus acousticus to the petrous apex under direct vision, (3) total exposure of the abducens nerve from the posterior fossa to its point of cross over the intracavernous carotid artery, and (4) wide extradural exposure of the cavernous carotid artery in the foramen lacerum region. This strategy can be combined with other related approaches; specifically, frontotemporal or posterior transpetrosal exposures for extensive lesions.
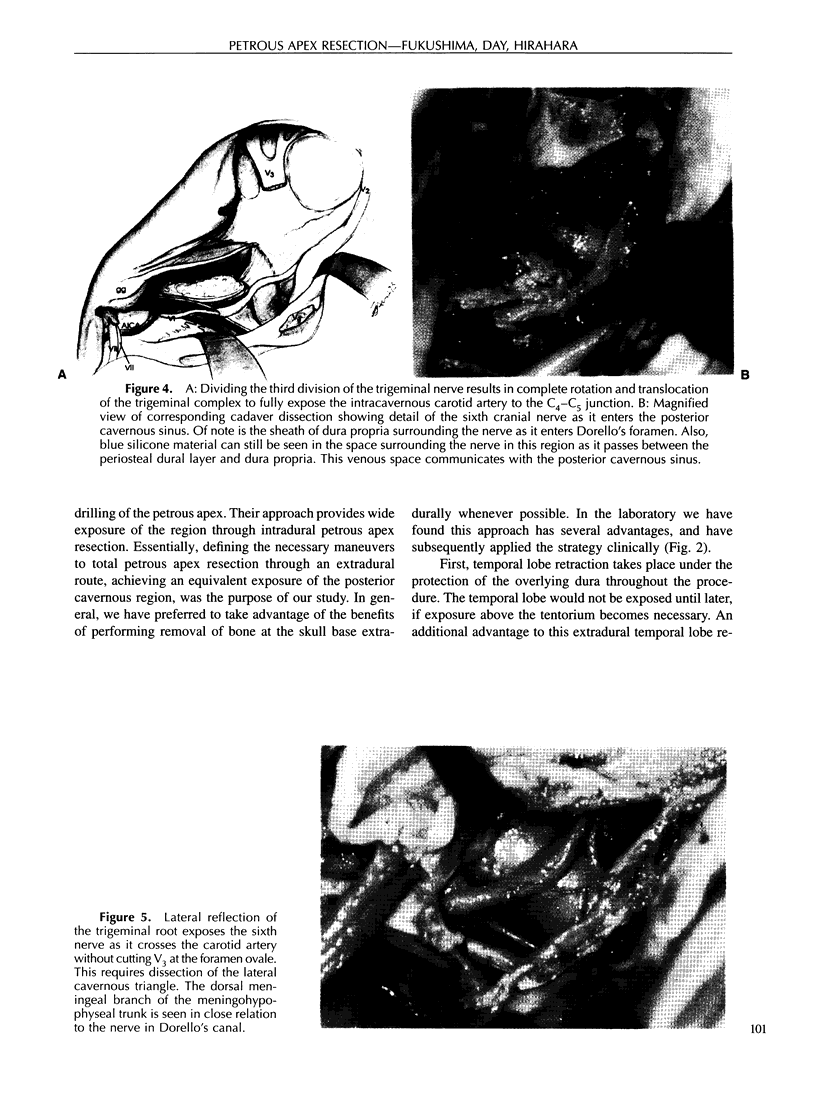
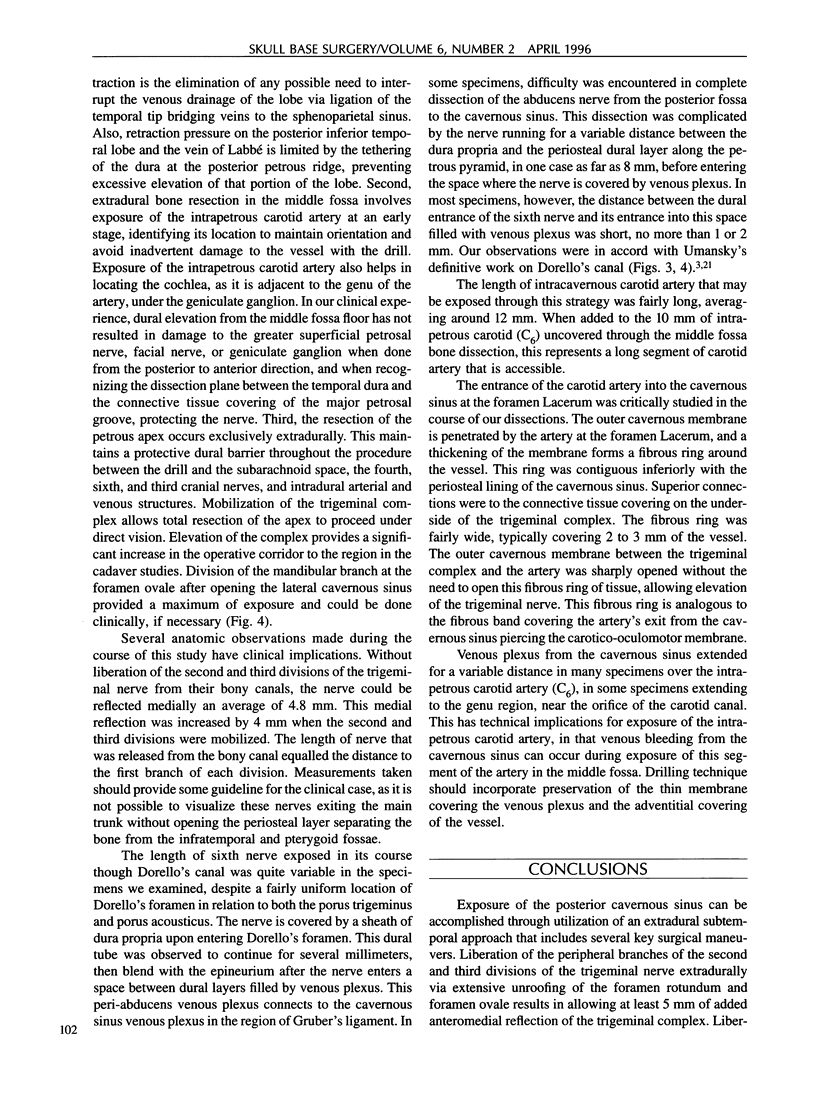
Microsurgical dissection and morphometric analysis were performed in 20 fixed cadaver specimens for the purposes of validating the method for clinical application and determining the key elements to maximization of exposure. The trigeminal complex could be anteromedially retracted 4.8 mm ± 1.3 (range = 3 to 6 mm) without skeletonization of V2 and V3. Liberating these two divisions from their bony canals to their first peripheral branch (10.4 mm ± 2.5 and 5.4 mm ± 1.1, respectively) resulted in increased mobilization an average of 9.1 mm ± 1.7 (7 to 14 mm). Further mobilization is achieved by dividing the attachment between the trigeminal connective tissue sheath and the fibrous carotid ring at the foramen lacerum. An average of 13.0 mm ± 3.1 (7 to 20 mm) of the posterior intracavernous carotid artery was exposed. Detailed microanatomic observations and a comprehensive morphometric analysis of the relevant anatomic relationships were made.
Full text
PDF



Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Al-Mefty O., Fox J. L., Smith R. R. Petrosal approach for petroclival meningiomas. Neurosurgery. 1988 Mar;22(3):510–517. doi: 10.1227/00006123-198803000-00010. [DOI] [PubMed] [Google Scholar]
- Dolenc V. Direct microsurgical repair of intracavernous vascular lesions. J Neurosurg. 1983 Jun;58(6):824–831. doi: 10.3171/jns.1983.58.6.0824. [DOI] [PubMed] [Google Scholar]
- Hakuba A., Nishimura S., Jang B. J. A combined retroauricular and preauricular transpetrosal-transtentorial approach to clivus meningiomas. Surg Neurol. 1988 Aug;30(2):108–116. doi: 10.1016/0090-3019(88)90095-x. [DOI] [PubMed] [Google Scholar]
- Harris F. S., Rhoton A. L. Anatomy of the cavernous sinus. A microsurgical study. J Neurosurg. 1976 Aug;45(2):169–180. doi: 10.3171/jns.1976.45.2.0169. [DOI] [PubMed] [Google Scholar]
- Harsh G. R., 4th, Sekhar L. N. The subtemporal, transcavernous, anterior transpetrosal approach to the upper brain stem and clivus. J Neurosurg. 1992 Nov;77(5):709–717. doi: 10.3171/jns.1992.77.5.0709. [DOI] [PubMed] [Google Scholar]
- Hitselberger W. E., Horn K. L., Hankinson H., Brackmann D. E., House W. F. The middle fossa transpetrous approach for petroclival meningiomas. Skull Base Surg. 1993;3(3):130–135. doi: 10.1055/s-2008-1060575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- House W. F., Hitselberger W. E., Horn K. L. The middle fossa transpetrous approach to the anterior-superior cerebellopontine angle. Am J Otol. 1986 Jan;7(1):1–4. [PubMed] [Google Scholar]
- House W. F., Hitselberger W. E. The transcochlear approach to the skull base. Arch Otolaryngol. 1976 Jun;102(6):334–342. doi: 10.1001/archotol.1976.00780110046004. [DOI] [PubMed] [Google Scholar]
- Kawase T., Shiobara R., Toya S. Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: surgical method and results in 10 patients. Neurosurgery. 1991 Jun;28(6):869–876. [PubMed] [Google Scholar]
- Spetzler R. F., Daspit C. P., Pappas C. T. The combined supra- and infratentorial approach for lesions of the petrous and clival regions: experience with 46 cases. J Neurosurg. 1992 Apr;76(4):588–599. doi: 10.3171/jns.1992.76.4.0588. [DOI] [PubMed] [Google Scholar]
- Umansky F., Elidan J., Valarezo A. Dorello's canal: a microanatomical study. J Neurosurg. 1991 Aug;75(2):294–298. doi: 10.3171/jns.1991.75.2.0294. [DOI] [PubMed] [Google Scholar]
- Umansky F., Nathan H. The lateral wall of the cavernous sinus. With special reference to the nerves related to it. J Neurosurg. 1982 Feb;56(2):228–234. doi: 10.3171/jns.1982.56.2.0228. [DOI] [PubMed] [Google Scholar]
- al-Mefty O., Ayoubi S., Smith R. R. The petrosal approach: indications, technique, and results. Acta Neurochir Suppl (Wien) 1991;53:166–170. doi: 10.1007/978-3-7091-9183-5_27. [DOI] [PubMed] [Google Scholar]