

Abstract
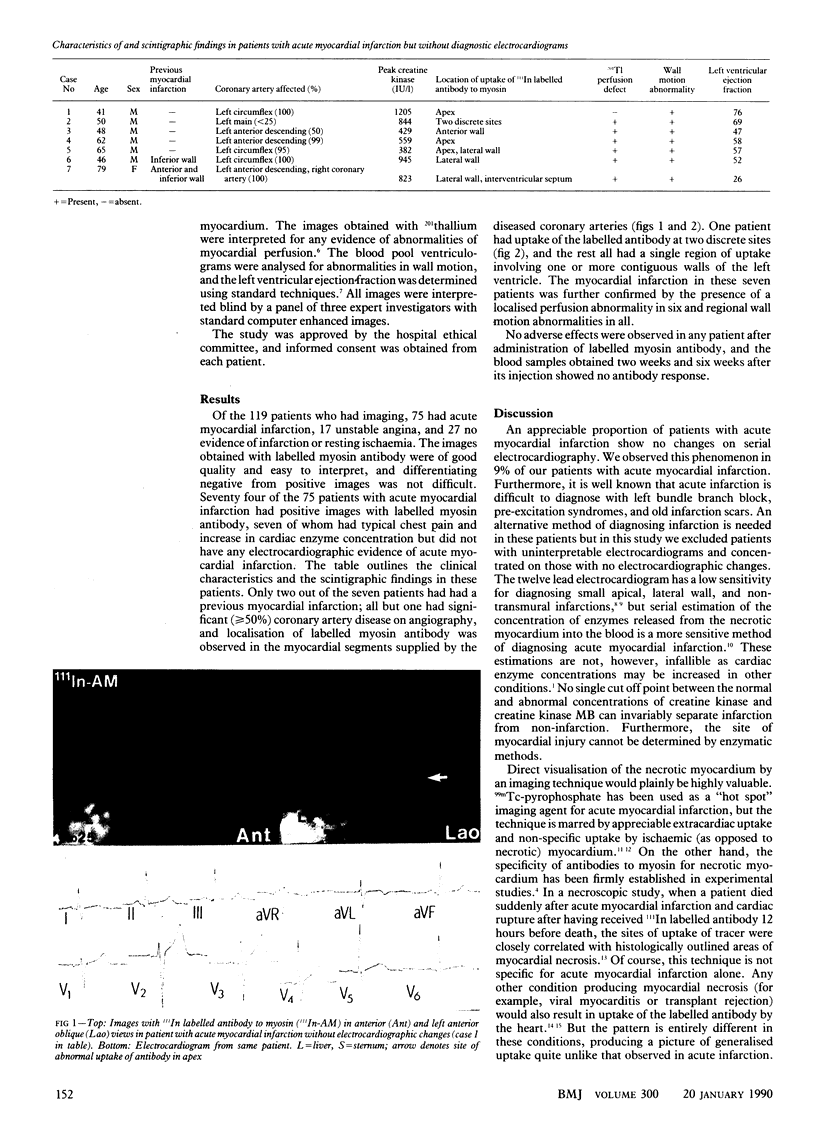
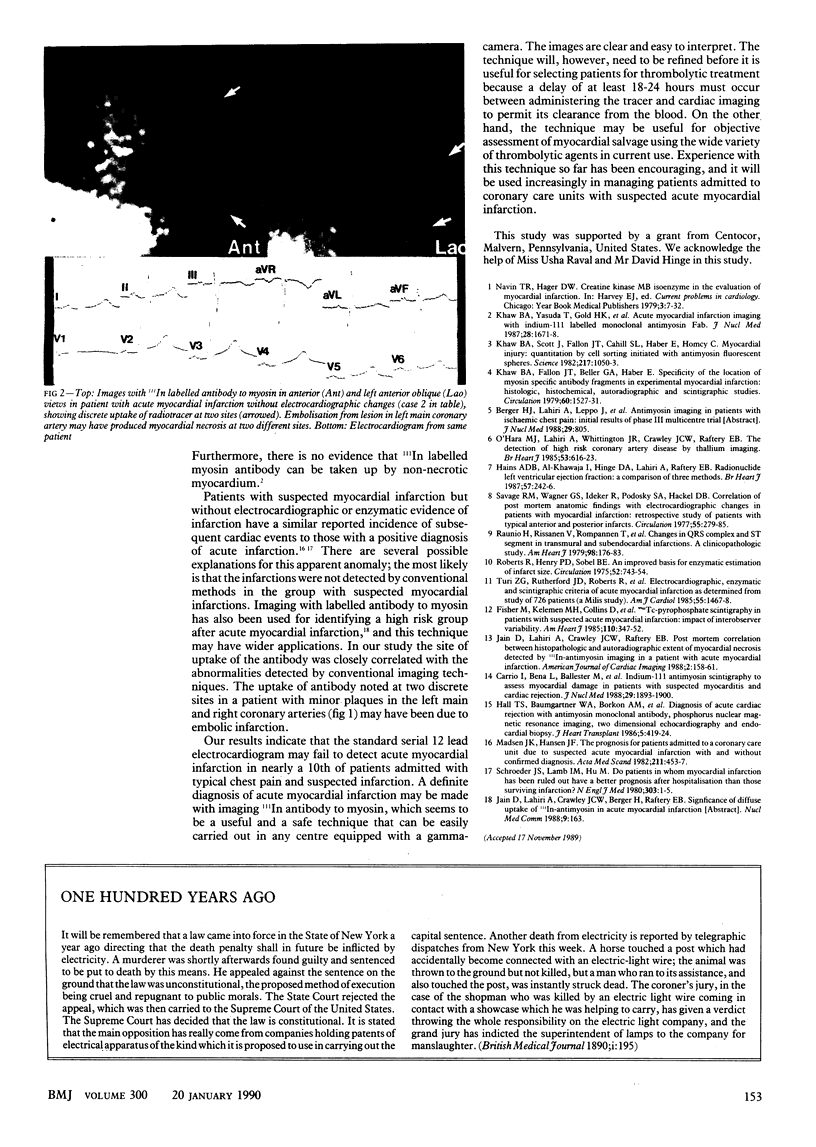
OBJECTIVE--To establish whether immunoscintigraphy with antibody to myosin may detect acute myocardial infarction without electrocardiographic changes. DESIGN--Prospective study of patients with suspected acute myocardial infarction or unstable angina with cardiac imaging with 111indium myosin antibody, estimation of cardiac enzyme concentrations, electrocardiography, 201thallium imaging, and radionuclide ventriculography. SETTING--Coronary care unit in a district general hospital. PATIENTS--119 Consecutive patients with suspected acute myocardial infarction or unstable angina. Patients with cardiomyopathy, myocarditis, valvular heart disease, myocardial infarction or cardiac surgery in the previous two weeks or with left bundle branch block and women of childbearing age were excluded. RESULTS--Of 75 patients with suspected acute myocardial infarction, seven had no diagnostic electrocardiographic changes despite normal conduction patterns. Immunoscintigraphy with myosin antibody disclosed necrosis in all seven patients, which was localised in regions supplied by diseased coronary arteries in all but one. Six patients had abnormal images on 201thallium imaging, and all seven had abnormal wall motion at the site of antibody uptake. One patient with minimal left main stem and right coronary artery atheroma had uptake of antibody at two discrete sites. CONCLUSIONS--Immunoscintigraphy with antibody to myosin confirms myocardial infarction in the absence of electrocardiographic changes and discloses the site of infarction.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Carrió I., Berná L., Ballester M., Estorch M., Obrador D., Cladellas M., Abadal L., Ginjaume M. Indium-111 antimyosin scintigraphy to assess myocardial damage in patients with suspected myocarditis and cardiac rejection. J Nucl Med. 1988 Dec;29(12):1893–1900. [PubMed] [Google Scholar]
- Fisher M. L., Kelemen M. H., Collins D., Holder L., Winzelberg G., Plotnick G. D., Morris F., Moran G. W., Carliner N. H., Peters R. W. Technetium-99m-pyrophosphate scintigraphy in patients with suspected acute myocardial infarction: impact of interobserver variability. Am Heart J. 1985 Aug;110(2):347–352. doi: 10.1016/0002-8703(85)90155-3. [DOI] [PubMed] [Google Scholar]
- Hains A. D., Al-Khawaja I., Hinge D. A., Lahiri A., Raftery E. B. Radionuclide left ventricular ejection fraction: a comparison of three methods. Br Heart J. 1987 Mar;57(3):242–246. doi: 10.1136/hrt.57.3.242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall T. S., Baumgartner W. A., Borkon A. M., LaFrance N. D., Traill T. A., Norris S., Hutchins G. M., Brawn J., Reitz B. A. Diagnosis of acute cardiac rejection with antimyosin monoclonal antibody, phosphorous nuclear magnetic resonance imaging, two-dimensional echocardiography, and endocardial biopsy. J Heart Transplant. 1986 Nov-Dec;5(6):419–424. [PubMed] [Google Scholar]
- Khaw B. A., Fallon J. T., Beller G. A., Haber E. Specificity of localization of myosin-specific antibody fragments in experimental myocardial infarction. Histologic, histochemical, autoradiographic and scintigraphic studies. Circulation. 1979 Dec;60(7):1527–1531. doi: 10.1161/01.cir.60.7.1527. [DOI] [PubMed] [Google Scholar]
- Khaw B. A., Scott J., Fallon J. T., Cahill S. L., Haber E., Homcy C. Myocardial injury: quantitation by cell sorting initiated with antimyosin fluorescent spheres. Science. 1982 Sep 10;217(4564):1050–1053. doi: 10.1126/science.7051286. [DOI] [PubMed] [Google Scholar]
- Khaw B. A., Yasuda T., Gold H. K., Leinbach R. C., Johns J. A., Kanke M., Barlai-Kovach M., Strauss H. W., Haber E. Acute myocardial infarct imaging with indium-111-labeled monoclonal antimyosin Fab. J Nucl Med. 1987 Nov;28(11):1671–1678. [PubMed] [Google Scholar]
- Kyst Madsen J., Fischer Hansen J. The prognosis for patients admitted to a coronary care unit due to suspected acute myocardial infarction with and without confirmed diagnosis. Acta Med Scand. 1982;211(6):453–457. doi: 10.1111/j.0954-6820.1982.tb01981.x. [DOI] [PubMed] [Google Scholar]
- O'Hara M. J., Lahiri A., Whittington J. R., Crawley J. C., Raftery E. B. Detection of high risk coronary artery disease by thallium imaging. Br Heart J. 1985 Jun;53(6):616–623. doi: 10.1136/hrt.53.6.616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raunio H., Rissanen V., Romppanen T., Jokinen Y., Rehnberg S., Helin M., Pyörälä K. Changes in the QRS complex and ST segment in transmural and subendocardial myocardial infarctions. A clinicopathologic study. Am Heart J. 1979 Aug;98(2):176–184. doi: 10.1016/0002-8703(79)90219-9. [DOI] [PubMed] [Google Scholar]
- Roberts R., Henry P. D., Sobel B. E. An improved basis for enzymatic estimation of infarct size. Circulation. 1975 Nov;52(5):743–754. doi: 10.1161/01.cir.52.5.743. [DOI] [PubMed] [Google Scholar]
- Savage R. M., Wagner G. S., Ideker R. E., Podolsky S. A., Hackel D. B. Correlation of postmortem anatomic findings with electrocardiographic changes in patients with myocardial infarction: retrospective study of patients with typical anterior and posterior infarcts. Circulation. 1977 Feb;55(2):279–285. doi: 10.1161/01.cir.55.2.279. [DOI] [PubMed] [Google Scholar]