

Abstract
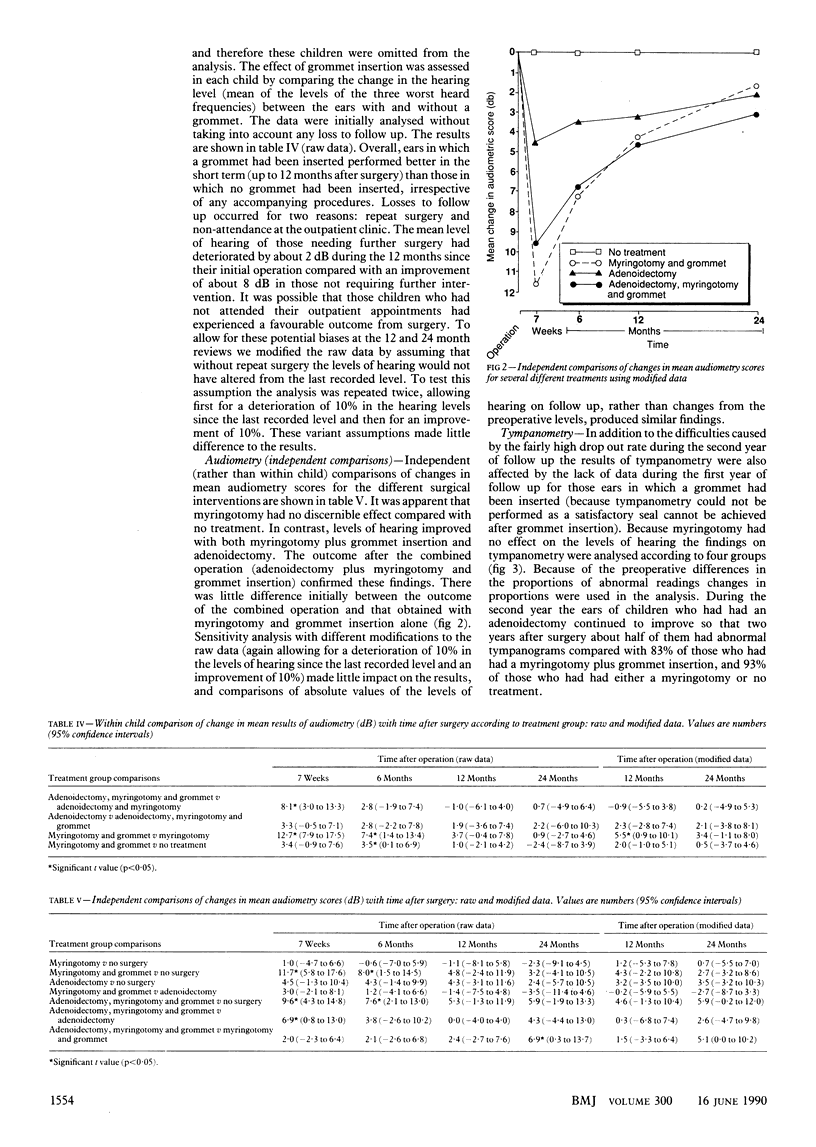
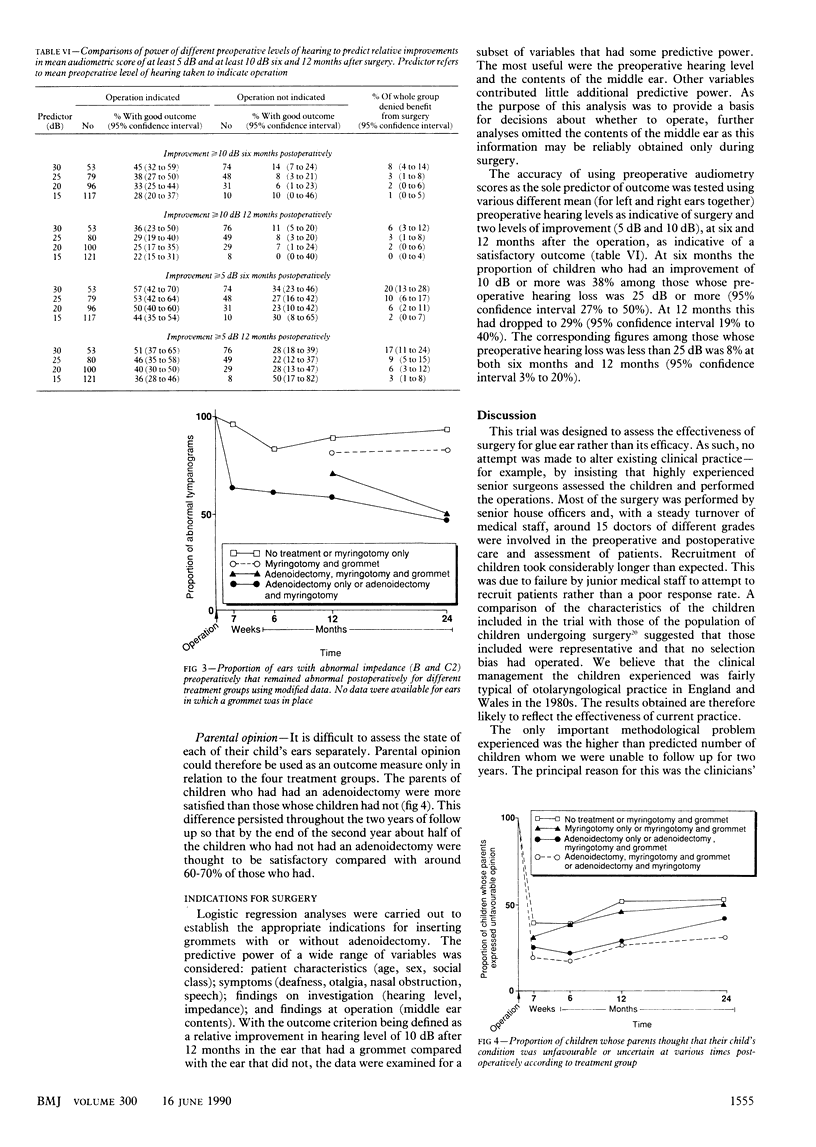
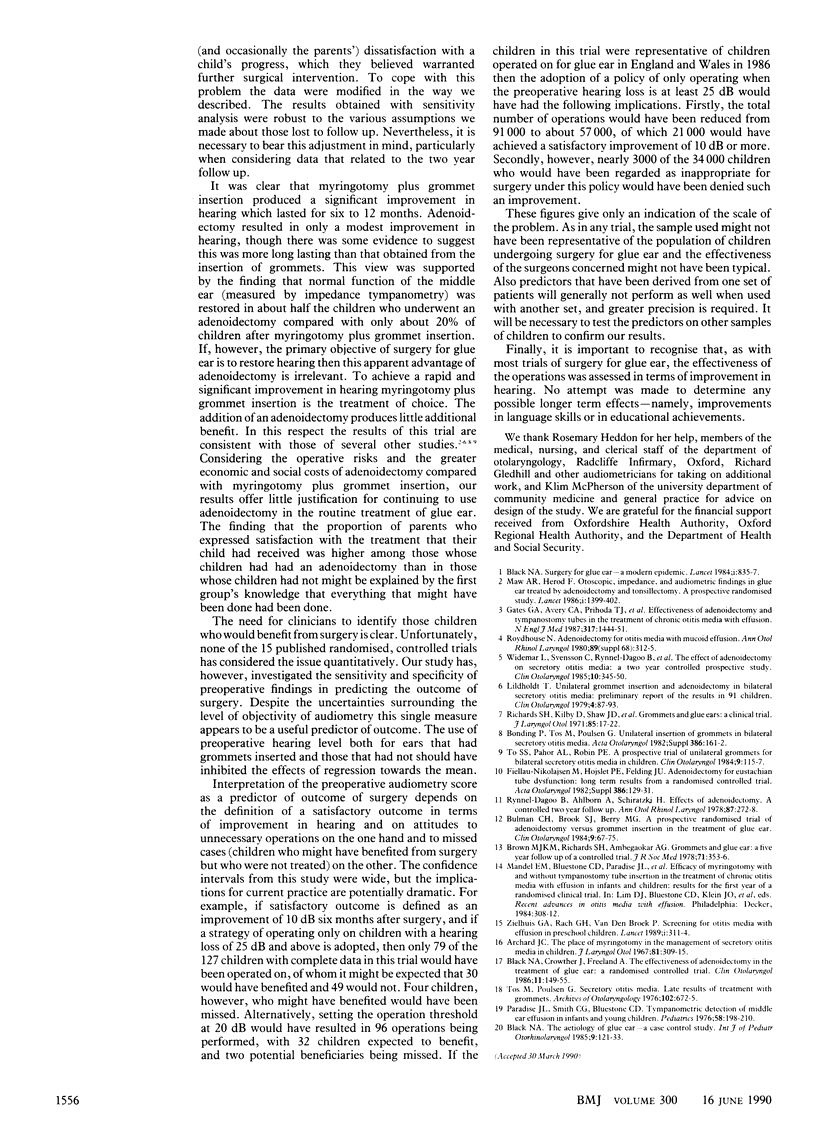
OBJECTIVE--To assess the effect of five different surgical treatments for glue ear (secretory otitis media) on improvement in hearing and, assuming one or more treatments to be effective, to identify the appropriate indications for surgery. DESIGN--Randomised controlled trial of children receiving (a) adenoidectomy, bilateral myringotomy, and insertion of a unilateral grommet; (b) adenoidectomy, unilateral myringotomy, and insertion of a unilateral grommet; (c) bilateral myringotomy and insertion of a unilateral grommet; and (d) unilateral myringotomy and insertion of a grommet. Children were followed up at seven weeks, six months, 12 months, and 24 months by symptom history and clinical investigations. SETTING--Otolaryngology department in an urban hospital. PATIENTS--149 Children aged 4-9 years who were admitted for surgery for glue ear and who had no history of previous operations on tonsils, adenoids, or ears and no evidence of sensorineural deafness. Inadequate follow up information on levels of hearing and on middle ear function was obtained from 22. MAIN OUTCOME MEASURES--Mean hearing loss (dB) of the three worst heard frequencies between 250 and 4000 Hz, results of impedance tympanometry, and parental views on their child's progress. RESULTS--In the 127 children for whom adequate information was available ears in which a grommet had been inserted performed better in the short term (for at least six months) than those in which no grommet had been inserted, irrespective of any accompanying procedure. Most of the benefit had disappeared by 12 months. Adenoidectomy produced a slight improvement that was not significant, though was sustained for at least two years. The ears of children who had had an adenoidectomy with myringotomy and grommet insertion, however, continued to improve so that two years after surgery about 50% had abnormal tympanometry compared with 83% of those who had had only myringotomy and grommet insertion, and 93% of the group that had had no treatment. Logistic regression analyses identified preoperative hearing level as the single best predictor of good outcome from surgery. Other variables contributed little additional predictive power. CONCLUSIONS--If the principal objective of surgery for glue ear is to restore hearing then our study shows that insertion of grommets is the treatment of choice. The addition of an adenoidectomy will increase the likelihood of restoration of normal function of the middle ear but will not improve hearing. When deciding appropriate indications for surgery, a balance has to be made between performing unnecessary operations and failing to treat patients who might benefit from surgical intervention. Preoperative audiometry scores might be the best predictor in helping to make this decision.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Archard J. C. The place of myringotomy in the management of secretory otitis media in children. J Laryngol Otol. 1967 Mar;81(3):309–315. doi: 10.1017/s0022215100067104. [DOI] [PubMed] [Google Scholar]
- Black N., Crowther J., Freeland A. The effectiveness of adenoidectomy in the treatment of glue ear: a randomized controlled trial. Clin Otolaryngol Allied Sci. 1986 Jun;11(3):149–155. doi: 10.1111/j.1365-2273.1986.tb00121.x. [DOI] [PubMed] [Google Scholar]
- Black N. Surgery for glue ear--a modern epidemic. Lancet. 1984 Apr 14;1(8381):835–837. doi: 10.1016/s0140-6736(84)92280-3. [DOI] [PubMed] [Google Scholar]
- Black N. The aetiology of glue ear--a case-control study. Int J Pediatr Otorhinolaryngol. 1985 Jul;9(2):121–133. doi: 10.1016/s0165-5876(85)80012-4. [DOI] [PubMed] [Google Scholar]
- Brown M. J., Richards S. H., Ambegaokar A. G. Grommets and glue ear: a five-year follow up of a controlled trial. J R Soc Med. 1978 May;71(5):353–356. doi: 10.1177/014107687807100508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bulman C. H., Brook S. J., Berry M. G. A prospective randomized trial of adenoidectomy vs grommet insertion in the treatment of glue ear. Clin Otolaryngol Allied Sci. 1984 Apr;9(2):67–75. doi: 10.1111/j.1365-2273.1984.tb01476.x. [DOI] [PubMed] [Google Scholar]
- DRY T. J. Thoracic pain in cardiovascular disease. Proc Staff Meet Mayo Clin. 1956 Jan 11;31(1):10–15. [PubMed] [Google Scholar]
- Gates G. A., Avery C. A., Prihoda T. J., Cooper J. C., Jr Effectiveness of adenoidectomy and tympanostomy tubes in the treatment of chronic otitis media with effusion. N Engl J Med. 1987 Dec 3;317(23):1444–1451. doi: 10.1056/NEJM198712033172305. [DOI] [PubMed] [Google Scholar]
- Lildholdt T. Unilateral grommet insertion and adenoidectomy in bilateral secretory otitis media: preliminary report of the results in 91 children. Clin Otolaryngol Allied Sci. 1979 Apr;4(2):87–93. doi: 10.1111/j.1365-2273.1979.tb01868.x. [DOI] [PubMed] [Google Scholar]
- Maw A. R., Herod F. Otoscopic, impedance, and audiometric findings in glue ear treated by adenoidectomy and tonsillectomy. A prospective randomised study. Lancet. 1986 Jun 21;1(8495):1399–1402. doi: 10.1016/s0140-6736(86)91552-7. [DOI] [PubMed] [Google Scholar]
- Paradise J. L., Smith C. G., Bluestone C. D. Tympanometric detection of middle ear effusion in infants and young children. Pediatrics. 1976 Aug;58(2):198–210. [PubMed] [Google Scholar]
- Richards S. H., Shaw J. D., Kilby D., Campbel H. Grommets and glue ears: a clinical trial. J Laryngol Otol. 1971 Jan;85(1):17–22. doi: 10.1017/s0022215100073096. [DOI] [PubMed] [Google Scholar]
- Rynnel-Dagö B., Ahlbom A., Schiratzki H. Effects of adenoidectomy: a controlled two-year follow-up. Ann Otol Rhinol Laryngol. 1978 Mar-Apr;87(2 Pt 1):272–278. doi: 10.1177/000348947808700223. [DOI] [PubMed] [Google Scholar]
- To S. S., Pahor A. L., Robin P. E. A prospective trial of unilateral grommets for bilateral secretory otitis media in children. Clin Otolaryngol Allied Sci. 1984 Apr;9(2):115–117. doi: 10.1111/j.1365-2273.1984.tb01483.x. [DOI] [PubMed] [Google Scholar]
- Widemar L., Svensson C., Rynnel-Dagö B., Schiratzki H. The effect of adenoidectomy on secretory otitis media: a 2-year controlled prospective study. Clin Otolaryngol Allied Sci. 1985 Dec;10(6):345–350. doi: 10.1111/j.1365-2273.1985.tb00267.x. [DOI] [PubMed] [Google Scholar]
- Zielhuis G. A., Rach G. H., van den Broek P. Screening for otitis media with effusion in preschool children. Lancet. 1989 Feb 11;1(8633):311–314. doi: 10.1016/s0140-6736(89)91317-2. [DOI] [PubMed] [Google Scholar]