

Abstract
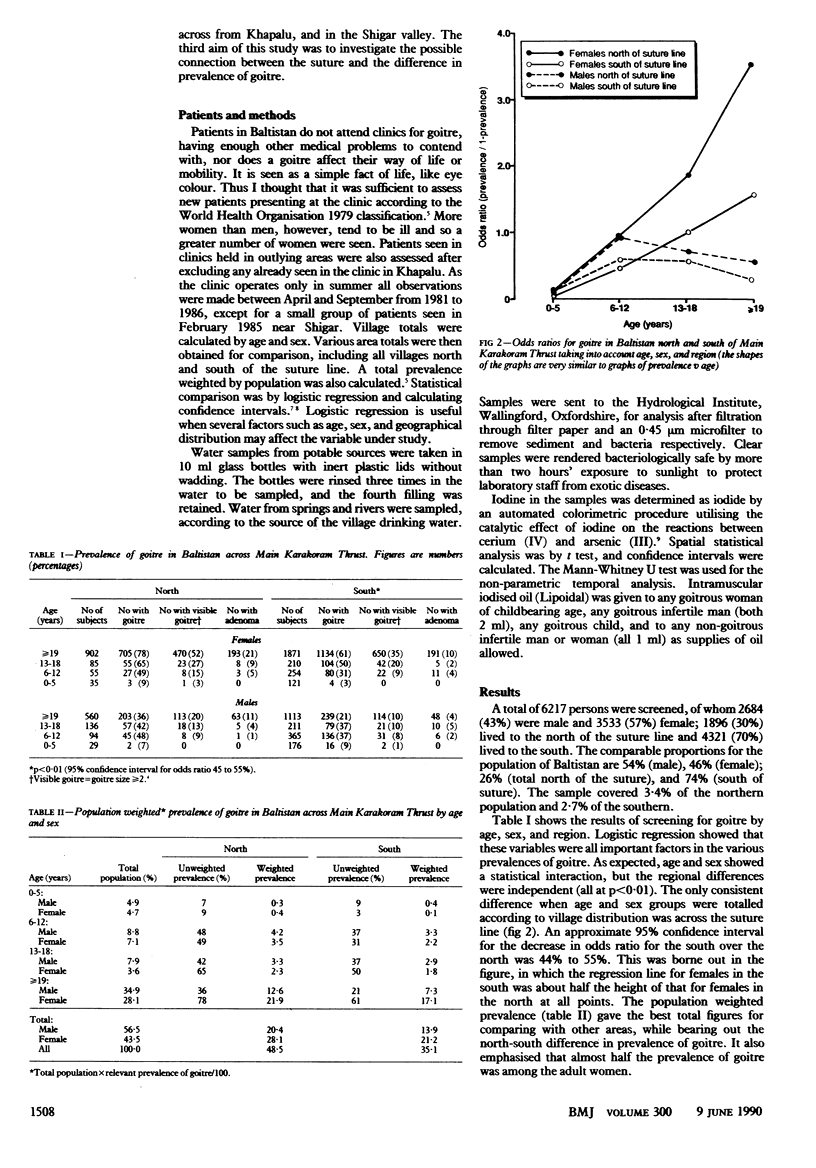
Although Baltistan, north east Pakistan, is in a region of iodine deficiency disorders, the distribution of goitre within the district, according to age and sex, has not been clearly defined. To establish the prevalence of the condition and to measure the reported difference in prevalence in the north and south of the district thyroid size was assessed in new patients attending the Aman clinic, Khapalu, and outlying areas between April and September from 1981 to 1986. Samples of potable water collected from villages were analysed for iodine (as iodide) concentrations in Britain. Population weighted prevalences were: in the north in males 20.4%, in females 28.1% and in the south in males 13.9%, in females 21.2%. There was an overall deficiency of iodine in the water (mean iodine (as iodide) concentrations (north) 11.0 nmol/l (1.4 micrograms/l), (south) 11.8 nmol/l (1.5 micrograms/l) (95% confidence interval -0.7 to 0.9). The differences followed the Main Karakoram Thrust, suggesting a geological goitrogen in the north, which might be minerals containing ions such as BF4- and SO3F-, and molybdenite and calcium, which are present in rocks in Baltistan. A new hypothesis for the genesis of endemic goitre is proposed--that is, that continents on crustal plates drift across the earth and collide, one plate sliding under the other and melting, giving rise to characteristic mineral assemblages in the overlying rocks. As the minerals weather out they enter the diet of the local population, where in the presence of iodine deficiency they produce or enhance iodine deficiency disorders. Despite the current iodised oil campaign by the Pakistani government with Unicef a long term working iodisation programme is still urgently needed.
Full text
PDF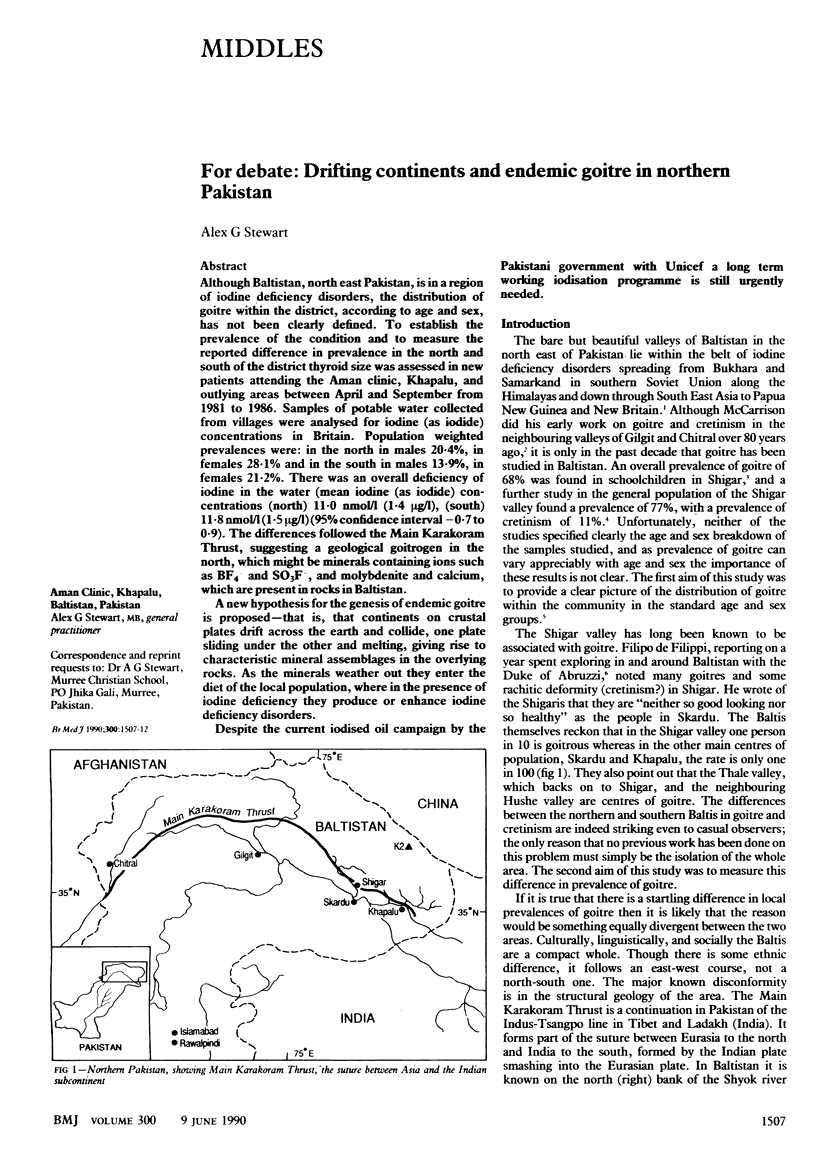

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Chapman J. A., Grant I. S., Taylor G., Mahmud K., Mulk S. U., Shahid M. A. Endemic goitre in the Gilgit Agency, West Pakistan with an appendix on dermatoglyphics and taste-testing. Philos Trans R Soc Lond B Biol Sci. 1972 Mar 23;263(856):459–490. doi: 10.1098/rstb.1972.0007. [DOI] [PubMed] [Google Scholar]
- Day T. K., Powell-Jackson P. R. Fluoride, water hardness, and endemic goitre. Lancet. 1972 May 27;1(7761):1135–1138. doi: 10.1016/s0140-6736(72)91370-0. [DOI] [PubMed] [Google Scholar]
- KELLY F. C., SNEDDEN W. W. Prevalence and geographical distribution of endemic goitre. Bull World Health Organ. 1958;18(1-2):5–173. [PMC free article] [PubMed] [Google Scholar]
- Karmarkar M. G., Deo M. G., Kochupillai N., Ramalingaswami V. Pathophysiology of Himalayan endemic goiter. Am J Clin Nutr. 1974 Jan;27(1):96–103. doi: 10.1093/ajcn/27.1.96. [DOI] [PubMed] [Google Scholar]
- RAMALINGASWAMI V., SUBRAMANIAN T. A., DEO M. G. The aetiology of Himalayan endemic goitre. Lancet. 1961 Apr 15;1(7181):791–794. doi: 10.1016/s0140-6736(61)90118-0. [DOI] [PubMed] [Google Scholar]
- WOLFF J. TRANSPORT OF IODIDE AND OTHER ANIONS IN THE THYROID GLAND. Physiol Rev. 1964 Jan;44:45–90. doi: 10.1152/physrev.1964.44.1.45. [DOI] [PubMed] [Google Scholar]
- White N. J. Nervous endemic cretinism in Eastern Nepal. Dev Med Child Neurol. 1977 Apr;19(2):208–212. doi: 10.1111/j.1469-8749.1977.tb07970.x. [DOI] [PubMed] [Google Scholar]