

Abstract
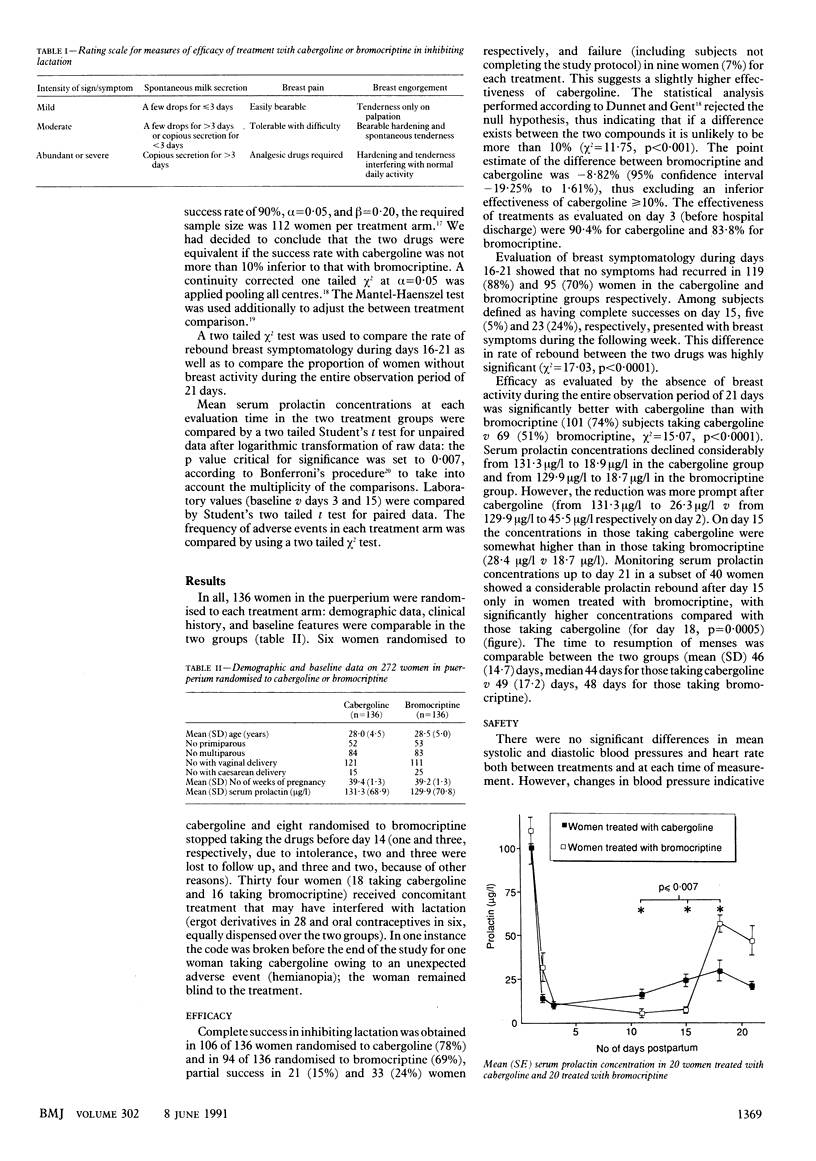
OBJECTIVE--To compare the efficacy and safety of a single dose of 1 mg of cabergoline with that of bromocriptine 2.5 mg twice daily for 14 days in the inhibition of puerperal lactation. DESIGN--Prospective, randomised, double blind, parallel group, multicentre study. SETTING--University of hospital departments of obstetrics and gynaecology in different European countries. SUBJECTS--272 puerperal women not wishing to lactate (136 randomised to each drug). INTERVENTIONS--Women randomised to cabergoline received two 0.5 mg tablets of cabergoline and one placebo tablet within 27 hours after delivery and then placebo twice daily for 14 days. Those randomised to bromocriptine received 2.5 mg of bromocriptine and two placebo tablets within 27 hours and then 2.5 mg of bromocriptine twice daily for 14 days. MAIN OUTCOME MEASURES--Success of treatment (complete or partial) according to milk secretion, breast engorgement, and breast pain; rebound symptomatology; serum prolactin concentrations; and number of adverse events. RESULTS--Complete success was achieved in 106 of 136 women randomised to cabergoline and in 94 of 136 randomised to bromocriptine and partial success in 21 and 33 women respectively. Rebound breast symptomatology occurred respectively in five and 23 women with complete success up to day 15 (p less than 0.0001). Serum prolactin concentrations dropped considerably with both drugs from day 2 to day 15; a prolactin secretion rebound effect was observed in women treated with bromocriptine. cabergoline and 36 receiving bromocriptine (p = 0.054), occurring most during the first treatment day. CONCLUSION--A single 1 mg dose of cabergoline is at least as effective as bromocriptine 2.5 mg twice daily for 14 days in preventing puerperal lactation. Because of the considerably lower rate of rebound breast activity and adverse events and the simpler administration schedule cabergoline should be the drug of choice for lactation inhibition.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Blackwelder W. C. "Proving the null hypothesis" in clinical trials. Control Clin Trials. 1982 Dec;3(4):345–353. doi: 10.1016/0197-2456(82)90024-1. [DOI] [PubMed] [Google Scholar]
- Crosignani P. G., Lombroso G. C., Caccamo A., Reschini E., Peracchi M. Suppression of puerperal lactation by metergoline. Obstet Gynecol. 1978 Jan;51(1):113–115. [PubMed] [Google Scholar]
- Daniel D. G., Campbell H., Turnbull A. C. Puerperal thromboembolism and suppression of lactation. Lancet. 1967 Aug 5;2(7510):287–289. doi: 10.1016/s0140-6736(67)90117-1. [DOI] [PubMed] [Google Scholar]
- Duchesne C., Leke R. Bromocriptine mesylate for prevention of postpartum lactation. Obstet Gynecol. 1981 Apr;57(4):464–467. [PubMed] [Google Scholar]
- Dunnett C. W., Gent M. Significance testing to establish equivalence between treatments, with special reference to data in the form of 2X2 tables. Biometrics. 1977 Dec;33(4):593–602. [PubMed] [Google Scholar]
- Ferrari C., Barbieri C., Caldara R., Mucci M., Codecasa F., Paracchi A., Romano C., Boghen M., Dubini A. Long-lasting prolactin-lowering effect of cabergoline, a new dopamine agonist, in hyperprolactinemic patients. J Clin Endocrinol Metab. 1986 Oct;63(4):941–945. doi: 10.1210/jcem-63-4-941. [DOI] [PubMed] [Google Scholar]
- Kochenour N. K. Lactation suppression. Clin Obstet Gynecol. 1980 Dec;23(4):1045–1059. doi: 10.1097/00003081-198012000-00008. [DOI] [PubMed] [Google Scholar]
- MANTEL N., HAENSZEL W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959 Apr;22(4):719–748. [PubMed] [Google Scholar]
- Melis G. B., Mais V., Paoletti A. M., Beneventi F., Gambacciani M., Fioretti P. Prevention of puerperal lactation by a single oral administration of the new prolactin-inhibiting drug, cabergoline. Obstet Gynecol. 1988 Mar;71(3 Pt 1):311–314. [PubMed] [Google Scholar]
- Peters F., Del Pozo E., Conti A., Breckwoldt M. Inhibition of lactation by a long-acting bromocriptine. Obstet Gynecol. 1986 Jan;67(1):82–85. [PubMed] [Google Scholar]
- Rolland R. Use of bromocriptine in the inhibition of puerperal lactation. Drugs. 1979 May;17(5):326–336. doi: 10.2165/00003495-197917050-00002. [DOI] [PubMed] [Google Scholar]
- Tindall V. R. Factors influencing puerperal thrombo-embolism. J Obstet Gynaecol Br Commonw. 1968 Dec;75(12):1324–1327. doi: 10.1111/j.1471-0528.1968.tb02952.x. [DOI] [PubMed] [Google Scholar]
- Van Dam L. J., Rolland R. Lactation-inhibiting and prolactin-lowering effect of lisuride and bromocriptine: a comparative study. Eur J Obstet Gynecol Reprod Biol. 1981 Nov;12(5):323–330. doi: 10.1016/0028-2243(81)90055-1. [DOI] [PubMed] [Google Scholar]