

Abstract
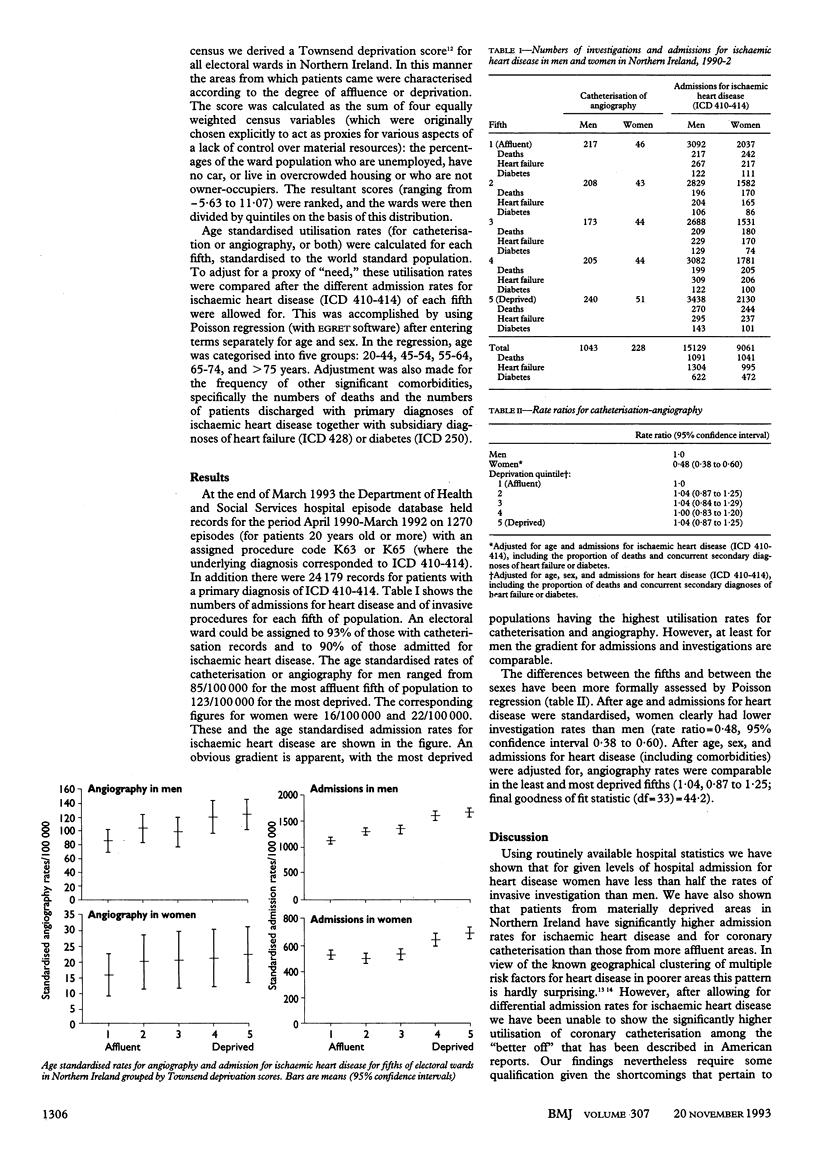
OBJECTIVE--To determine the effects of patient's sex and area's material deprivation on utilisation rates of coronary catheterisation and angiography in the investigation of ischaemic heart disease. DESIGN--Retrospective analysis of routinely collected hospital statistics. SETTING--Acute hospitals throughout Northern Ireland. SUBJECTS--24,179 episodes of patients discharged from hospital with a primary diagnosis of ischaemic heart disease and 1270 episodes relating to patients with an underlying diagnosis of ischaemic heart disease who had either coronary catheterisation or angiography. MAIN OUTCOME MEASURES--Age standardised admission rates for heart disease and age standardised utilisation rates for catheterisation or angiography, or both, for 566 electoral wards ranked by Townsend "deprivation" scores. RESULTS--Catheterisation-angiography rates in men were over fivefold those of women, ranging from 85.5/100,000 v 16/100,000 in patients from "well off" areas to 123/100,000 v 22/100,000 for patients from deprived areas. After admission rates for heart disease were controlled for, the overall rate ratio for women was 0.48 (95% confidence interval 0.38 to 0.60). After differential admission rates for heart disease and other potential clinical confounders were controlled for, the investigation rates of patients from the least and most "deprived" areas were not significantly different (rate ratio 1.04 (0.87 to 1.25)). CONCLUSION--Although investigation rates were significantly lower in women than in men, further clinical data would be required before labelling this underutilisation as evidence of bias. There was no significant difference in invasive investigation rates for heart disease in areas of varying deprivation or affluence.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bernstein S. J., Hilborne L. H., Leape L. L., Fiske M. E., Park R. E., Kamberg C. J., Brook R. H. The appropriateness of use of coronary angiography in New York State. JAMA. 1993 Feb 10;269(6):766–769. [PubMed] [Google Scholar]
- Bernstein S. J., Kosecoff J., Gray D., Hampton J. R., Brook R. H. The appropriateness of the use of cardiovascular procedures. British versus U.S. perspectives. Int J Technol Assess Health Care. 1993 Winter;9(1):3–10. doi: 10.1017/s0266462300002981. [DOI] [PubMed] [Google Scholar]
- Bickell N. A., Pieper K. S., Lee K. L., Mark D. B., Glower D. D., Pryor D. B., Califf R. M. Referral patterns for coronary artery disease treatment: gender bias or good clinical judgment? Ann Intern Med. 1992 May 15;116(10):791–797. doi: 10.7326/0003-4819-116-10-791. [DOI] [PubMed] [Google Scholar]
- Bobbio M., Detrano R., Shandling A. H., Ellestad M. H., Clark J., Brezden O., Abecia A., Martinez-Caro D. Clinical assessment of the probability of coronary artery disease: judgmental bias from personal knowledge. Med Decis Making. 1992 Jul-Sep;12(3):197–203. doi: 10.1177/0272989X9201200305. [DOI] [PubMed] [Google Scholar]
- Crombie I. K., Kenicer M. B., Smith W. C., Tunstall-Pedoe H. D. Unemployment, socioenvironmental factors, and coronary heart disease in Scotland. Br Heart J. 1989 Feb;61(2):172–177. doi: 10.1136/hrt.61.2.172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crombie I. K., Smith W. C., Tavendale R., Tunstall-Pedoe H. Geographical clustering of risk factors and lifestyle for coronary heart disease in the Scottish Heart Health Study. Br Heart J. 1990 Sep;64(3):199–203. doi: 10.1136/hrt.64.3.199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtis S. E. Use of survey data and small area statistics to assess the link between individual morbidity and neighbourhood deprivation. J Epidemiol Community Health. 1990 Mar;44(1):62–68. doi: 10.1136/jech.44.1.62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elder A. T., Shaw T. R., Turnbull C. M., Starkey I. R. Elderly and younger patients selected to undergo coronary angiography. BMJ. 1991 Oct 19;303(6808):950–953. doi: 10.1136/bmj.303.6808.950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fiebach N. H., Viscoli C. M., Horwitz R. I. Differences between women and men in survival after myocardial infarction. Biology or methodology? JAMA. 1990 Feb 23;263(8):1092–1096. [PubMed] [Google Scholar]
- Garber C. E., Carleton R. A., Heller G. V. Comparison of "Rose Questionnaire Angina" to exercise thallium scintigraphy: different findings in males and females. J Clin Epidemiol. 1992 Jul;45(7):715–720. doi: 10.1016/0895-4356(92)90048-r. [DOI] [PubMed] [Google Scholar]
- Gordon A., Collin J. Save the normal foreskin. BMJ. 1993 Jan 2;306(6869):1–2. doi: 10.1136/bmj.306.6869.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gray D., Hampton J. R., Bernstein S. J., Kosecoff J., Brook R. H. Audit of coronary angiography and bypass surgery. Lancet. 1990 Jun 2;335(8701):1317–1320. doi: 10.1016/0140-6736(90)91196-h. [DOI] [PubMed] [Google Scholar]
- Lerner D. J., Kannel W. B. Patterns of coronary heart disease morbidity and mortality in the sexes: a 26-year follow-up of the Framingham population. Am Heart J. 1986 Feb;111(2):383–390. doi: 10.1016/0002-8703(86)90155-9. [DOI] [PubMed] [Google Scholar]
- Mays N., Chinn S. Relation between all cause standardised mortality ratios and two indices of deprivation at regional and district level in England. J Epidemiol Community Health. 1989 Jun;43(2):191–199. doi: 10.1136/jech.43.2.191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orencia A., Bailey K., Yawn B. P., Kottke T. E. Effect of gender on long-term outcome of angina pectoris and myocardial infarction/sudden unexpected death. JAMA. 1993 May 12;269(18):2392–2397. [PubMed] [Google Scholar]
- Park R. E., Fink A., Brook R. H., Chassin M. R., Kahn K. L., Merrick N. J., Kosecoff J., Solomon D. H. Physician ratings of appropriate indications for three procedures: theoretical indications vs indications used in practice. Am J Public Health. 1989 Apr;79(4):445–447. doi: 10.2105/ajph.79.4.445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Price C. E., Paul E. A., Bevan R. G., Holland W. W. Equity and medical practice variation: relationships between standardised discharge ratios in total and for selected conditions in English districts. J Epidemiol Community Health. 1992 Feb;46(1):58–62. doi: 10.1136/jech.46.1.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sox H. C., Jr, Hickam D. H., Marton K. I., Moses L., Skeff K. M., Sox C. H., Neal E. A. Using the patient's history to estimate the probability of coronary artery disease: a comparison of primary care and referral practices. Am J Med. 1990 Jul;89(1):7–14. doi: 10.1016/0002-9343(90)90090-z. [DOI] [PubMed] [Google Scholar]
- Tofler G. H., Muller J. E., Stone P. H., Davies G., Davis V. G., Braunwald E. Comparison of long-term outcome after acute myocardial infarction in patients never graduated from high school with that in more educated patients. Multicenter Investigation of the Limitation of Infarct Size (MILIS). Am J Cardiol. 1993 May 1;71(12):1031–1035. doi: 10.1016/0002-9149(93)90568-w. [DOI] [PubMed] [Google Scholar]
- Tunis S. R., Bass E. B., Klag M. J., Steinberg E. P. Variation in utilization of procedures for treatment of peripheral arterial disease. A look at patient characteristics. Arch Intern Med. 1993 Apr 26;153(8):991–998. [PubMed] [Google Scholar]
- Williams R. B., Barefoot J. C., Califf R. M., Haney T. L., Saunders W. B., Pryor D. B., Hlatky M. A., Siegler I. C., Mark D. B. Prognostic importance of social and economic resources among medically treated patients with angiographically documented coronary artery disease. JAMA. 1992 Jan 22;267(4):520–524. [PubMed] [Google Scholar]