

As of December 2000, the US census indicated that more than 8.7 million people of Mexican origin resided in California, with economic and social factors being the driving force for migration.[1] Baja California is a leading point of entry to the United States, with the Tijuana-San Diego border crossing being the busiest land port of entry in the world, with more than 131,000 legal border crossings daily. Therefore, Tijuana offers a unique opportunity to study the risk factors for HIV acquisition and migration patterns at the Mexico-US border.
Beginning in 1997, the University of California San Diego Mother, Child and Adolescent HIV Program established a collaboration with pediatricians and obstetricians who provide HIV care in Tijuana, Baja California, Mexico.[2] We recently conducted a cross-sectional study to evaluate the feasibility and acceptance of counseling and rapid HIV testing during pregnancy at Tijuana General Hospital.[3] Part of our study focused on internal migration patterns and risk factors for HIV acquisition. Between September and December 2003, information on residence during the previous 5 years was available for 1496 pregnant women at Tijuana General Hospital. Of these, 1017 resided in Tijuana in the previous 5 years, whereas 479 resided in other states in the previous 5 years, most of whom migrated from Sinaloa, Michoacan, Jalisco, Chiapas, and other cities in Baja California (Figure).
Figure.
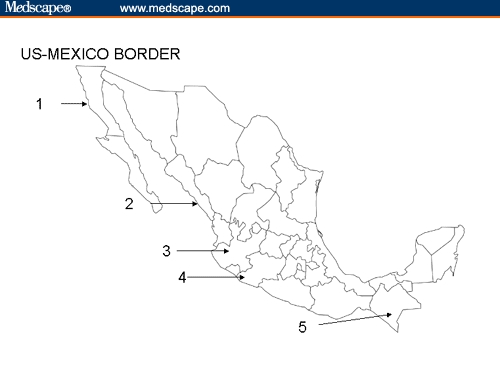
Map of Mexico. States of origin of migrating pregnant women, Tijuana General Hospital 2003. 1 indicates Baja California; 2, Sinaloa; 3, Jalisco; 4, Michoacan; and 5, Chiapas.
Migrants were defined as women who had resided in Tijuana for less than 5 years, whereas Tijuana residents were defined as those living in Tijuana for the previous 5 years. Migrants and Tijuana residents were similar with regard to marital status, mean number of lifetime sex partners, having ≥ 5 lifetime sex partners, number of prenatal care visits, and having a spouse or partner with prior blood transfusions or a spouse or partner who had sex with men. Tijuana residents were older (27.0 vs 25.1 years; P = .04), more likely to use injection drugs (7.4% vs 4.0%; P = .011) or other drugs (10.7% vs 6.9%; P = .018), more likely to have received a blood transfusion (11.9% vs 7.9%; P = .03), and were more likely to have a spouse or partner who uses injection drugs (12.5% vs 7.1%; P = .007) or other drugs (32.8% vs 21.7%; P 0002) (chi-square test). HIV prevalence did not differ among migrants (7 of 479; 1.46%) and Tijuana residents (7 of 1017; 0.69%) (P = .16, Fisher's exact test). The modes of HIV acquisition among the 14 HIV-infected pregnant women were as follows: injection drugs for 2 women (1 received a blood transfusion), other drugs (predominantly crystal methamphetamine) for 5 women, spouse received a blood transfusion for 1 woman, spouse used other drugs for 1 woman, spouse had sex with other women for 2 women, and no risk factors were identified for 3 women.
The HIV prevalence among pregnant Tijuana residents was found to be 10 times higher than the HIV prevalence in pregnancy reported by the Mexican National Center for HIV/AIDS Prevention and Control (CENSIDA) in other areas of Mexico, which is 0.09%.[4] This discrepancy may be explained by the nature of the population studied. Our study was hospital based, with 24% of our patients having no prenatal care before delivery and 54% having 2 or fewer prenatal visits; therefore, this was a high-risk population.[3] In contrast, the CENSIDA surveillance studies were conducted between 1990 and 1999 among women accessing prenatal care clinics; therefore, these women were at lower risk for HIV acquisition.[5] Furthermore, our studies that documented higher HIV prevalence in Tijuana pregnant residents may reflect an emerging phenomenon.[2,3]
Our study suggests that 32% of pregnant women who give birth at Tijuana General Hospital have recently migrated from other Mexican cities or states and their HIV seroprevalence is similar to the pregnant women who are long-term Tijuana residents. However, Tijuana residents were significantly more likely to engage in high-risk behavior for HIV acquisition. Although our study did not address the intention of these migrant women to return to their home communities, HIV surveillance is needed in these communities. In our study, migration was not associated with risk of HIV acquisition; however, studies in South Africa had found a higher rate of HIV infection among women who migrate to urban settings.[6]
We believe that our finding of high HIV seroprevalence among pregnant women who are long-term Tijuana residents and those who recently migrated to Tijuana from various Mexican states emphasizes the need for continued HIV surveillance and implementation of preventive interventions throughout Mexico. Further research is needed in other at risk populations in Tijuana and other border cities throughout the US-Mexico border.
Funding information
Supported by the NIH CFAR Supplement 2 P30 AI36214-09A1, State of California's University-wide AIDS Research Program IS02 SD 701 and ID03 SD 029, and AI3614 (Virology Core of the UCSD Center for AIDS Research). Also partially supported by the San Diego EXPORT Center, National Center of Minority Health and Health Disparities, NIH P60 MD00220
Contributor Information
Rolando M. Viani, Department of Pediatrics, Division of Infectious Diseases, University of California San Diego, School of Medicine, San Diego, California.
Maria Rosario G. Araneta, Department of Pediatrics and Family Medicine, University of California San Diego, School of Medicine, San Diego, California.
Jorge Ruiz-Calderon, Department of Obstetrics and Gynecology, Tijuana General Hospital, Tijuana, Mexico.
Patricia Hubbard, UCSD Mother Child and Adolescent HIV Program, San Diego, California.
Graciano Lopez, Department of Pediatrics, Tijuana General Hospital, Tijuana, Mexico.
Enrique Chacón-Cruz, Department of Pediatrics, Tijuana General Hospital, Tijuana, Mexico.
Stephen A. Spector, Department of Pediatrics, Division of Infectious Diseases, University of California San Diego, School of Medicine, San Diego, California.
References
- 1.US Census Bureau. United States Census 2000 report. Available at: http://wwwcensus.gov/Press-Release/www/2001/sumfile1.html. Accessed November 16, 2004.
- 2.Viani RM, Ruiz-Calderon J, Van Pratt C, Lopez G, Spector SA. HIV prevalence during pregnancy in Tijuana, Baja California, Mexico. AIDS. 2003;17:1113–1114. doi: 10.1097/00002030-200305020-00033. [DOI] [PubMed] [Google Scholar]
- 3.Viani RM, Araneta MR, Ruiz-Calderon J, et al. HIV-1 infection in a cohort of pregnant Women in Baja California, Mexico: evidence of an emerging crisis?. [ThPeC7301]; Program and abstracts of the XV International AIDS Conference; July 11–16, 2004; Bangkok, Thailand. [Google Scholar]
- 4.CENSIDA, Panorama Epidemiologico del VIH/SIDA e ITS en Mexico. 2004, Secretaria de Salud, Mexico City, Mexico; 2004. Available at: http://www.salud.gob.Mx/C0NASIDA Accessed September 30, 2004.
- 5.del Rio C, Sepúlveda J. AIDS in Mexico: lessons learned and implications for developing countries. AIDS. 2002;16:1445–1457. doi: 10.1097/00002030-200207260-00001. [DOI] [PubMed] [Google Scholar]
- 6.Zuma K, Gouws E, Williams B, Lurie M. Risk factors for HIV infection among women in Carletonville, South Africa: migration, demography and sexually transmitted diseases. Int J STD AIDS. 2003;14:814–817. doi: 10.1258/095646203322556147. [DOI] [PubMed] [Google Scholar]