

Abstract
Background—Wallstents (Schneider Stent, Inc., USA) used for the palliation of malignant biliary strictures, although associated with prolonged patency, can occlude. There is no consensus regarding the optimal management of Wallstent occlusion. Aims—To evaluate the efficacy of different endoscopic methods for managing biliary Wallstent occlusion. Methods—A multicentre retrospective study of patients managed for a biliary Wallstent occlusion. Results—Data were available for 38 patients with 44 Wallstent occlusions, all of which had initial endoscopic management. Twenty four patients had died and 14 were alive after a median follow up of 231 (30-1095) days following Wallstent occlusion. Occlusions were managed by insertion of another Wallstent in 19,insertion of a plastic stent in 20, and mechanical cleaning in five. Endoscopic management was successful in 43 (98%). Following management of the occlusion, bilirubin decreased from 6.0 (0.5-34.3) to 2.1 (0.2-27.7) mg/100 ml (p<0.05). No complications occurred. The median duration of second stent patency was 75 days (95% confidence interval 43 to 107) after insertion of another Wallstent, 90 days (71 to 109) after insertion of a plastic stent, and 34 days (30to 38) after mechanical cleaning (NS). The respective median survivals were 70 days (22-118), 98 days (54-142), and 34 days (30-380) (NS). Incremental cost effective analysis showed that plastic stent insertion is the most cost effective option. Conclusion—Although all three methods are equally effective in managing an occluded Wallstent, the most cost effective method appears to be plastic stent insertion.
Keywords: self expanding metal stent; biliary strictures; stent occlusion; jaundice; gastrointestinal malignancy
Full Text
The Full Text of this article is available as a PDF (143.9 KB).
Figure 1 .
Tumour ingrowth within a Wallstent.
Figure 2 .

Tumour overgrowth proximal to a Wallstent.
Figure 3 .

Debris within a Wallstent causing an obstruction. The debris was extracted using a balloon (mechanical cleaning).
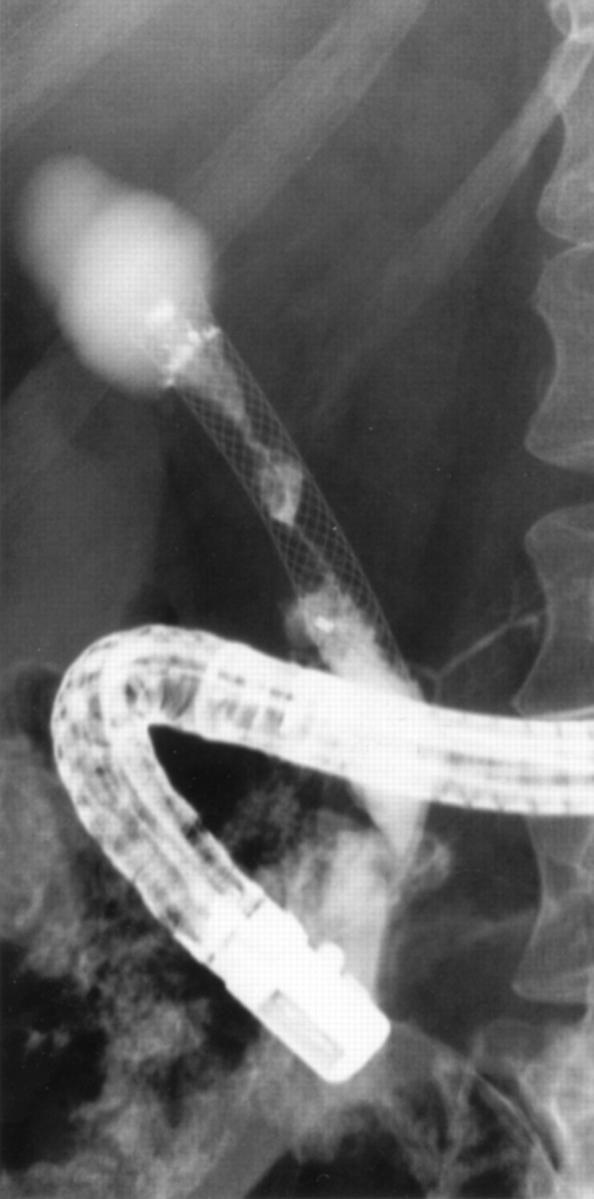
Figure 4 .

Second Wallstent inserted for occlusion of the first Wallstent showing good patency after deployment.
Figure 5 .

Two plastic stents inserted for occlusion of a Wallstent.
Figure 6 .

Overall patient survival following treatment of the first Wallstent occlusion.
Figure 7 .

Cumulative patency of Wallstent following treatment of the occlusion.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cotton P. B., Lehman G., Vennes J., Geenen J. E., Russell R. C., Meyers W. C., Liguory C., Nickl N. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991 May-Jun;37(3):383–393. doi: 10.1016/s0016-5107(91)70740-2. [DOI] [PubMed] [Google Scholar]
- Cremer M., Deviere J., Sugai B., Baize M. Expandable biliary metal stents for malignancies: endoscopic insertion and diathermic cleaning for tumor ingrowth. Gastrointest Endosc. 1990 Sep-Oct;36(5):451–457. doi: 10.1016/s0016-5107(90)71113-3. [DOI] [PubMed] [Google Scholar]
- Davids P. H., Groen A. K., Rauws E. A., Tytgat G. N., Huibregtse K. Randomised trial of self-expanding metal stents versus polyethylene stents for distal malignant biliary obstruction. Lancet. 1992 Dec 19;340(8834-8835):1488–1492. doi: 10.1016/0140-6736(92)92752-2. [DOI] [PubMed] [Google Scholar]
- Detsky A. S., Naglie I. G. A clinician's guide to cost-effectiveness analysis. Ann Intern Med. 1990 Jul 15;113(2):147–154. doi: 10.7326/0003-4819-113-2-147. [DOI] [PubMed] [Google Scholar]
- Ell C., Fleig W. E., Hochberger J. Broken biliary metal stent after repeated electrocoagulation for tumor ingrowth. Gastrointest Endosc. 1992 Mar-Apr;38(2):197–199. doi: 10.1016/s0016-5107(92)70396-4. [DOI] [PubMed] [Google Scholar]
- Goldin E., Beyar M., Safra T., Globerman O., Verstandig A., Wengrower D., Fich A. A new self-expandable and removable metal stent for biliary obstruction--a preliminary report. Endoscopy. 1993 Nov;25(9):597–599. doi: 10.1055/s-2007-1010412. [DOI] [PubMed] [Google Scholar]
- Lossef S. V., Druy E., Jelinger E., Fleischer D., Barth K. H. Use of hot-tip laser probes to recanalize occluded expandable metallic biliary endoprostheses. AJR Am J Roentgenol. 1992 Jan;158(1):199–201. doi: 10.2214/ajr.158.1.1309219. [DOI] [PubMed] [Google Scholar]
- Mixon T., Goldschmid S., Brady P. G., Boulay J. Endoscopic management of expandable metallic biliary stent occlusion. Gastrointest Endosc. 1993 Jan-Feb;39(1):82–84. doi: 10.1016/s0016-5107(93)70020-6. [DOI] [PubMed] [Google Scholar]
- Schmassmann A., von Gunten E., Knuchel J., Scheurer U., Fehr H. F., Halter F. Wallstents versus plastic stents in malignant biliary obstruction: effects of stent patency of the first and second stent on patient compliance and survival. Am J Gastroenterol. 1996 Apr;91(4):654–659. [PubMed] [Google Scholar]
- Silvis S. E., Sievert C. E., Jr, Vennes J. A., Abeyta B. K., Brennecke L. H. Comparison of covered versus uncovered wire mesh stents in the canine biliary tract. Gastrointest Endosc. 1994 Jan-Feb;40(1):17–21. doi: 10.1016/s0016-5107(94)70004-4. [DOI] [PubMed] [Google Scholar]
- Speer A. G., Cotton P. B., Rode J., Seddon A. M., Neal C. R., Holton J., Costerton J. W. Biliary stent blockage with bacterial biofilm. A light and electron microscopy study. Ann Intern Med. 1988 Apr;108(4):546–553. doi: 10.7326/0003-4819-108-4-546. [DOI] [PubMed] [Google Scholar]