

Abstract
Dextrocardia is a rare clinical phenomenon with a reported incidence of one in 10 000. Consequently, acute coronary syndromes in such patients are rare. When chest pain occurs in this setting, it is important to be aware of the unique problems that may occur if coronary intervention is contemplated. Previous case reports have shown successful attempts at reperfusing one coronary artery percutaneously. In this case, coronary stents were successfully deployed in two vessels of a man with situs inversus, which has not been reported before. Additionally, the angiographic results that followed from successful intervention did not produce the expected haemodynamic and electrocardiographic changes.
Keywords: situs inversus, acute coronary syndrome, dextrocardia
A 67 year old man presented with chest pain at rest. He was a smoker with a family history of ischaemic heart disease. He was known to have situs inversus but not bronchiectasis. Clinically his apex beat was right sided, with a left sided liver and a right sided spleen. Chest radiography confirmed the presence of a right sided stomach gas bubble and a right sided aortic knuckle (fig 1).
Figure 1.

Chest radiograph confirming the presence of a right sided stomach gas bubble and a right sided aortic knuckle.
His surface ECG showed inferior ST elevation and anterior ST depression with low R wave voltages in the anterolateral leads when conventional lead placement was used. After chest leads were placed on the right side and limb leads were reversed the inferior ST elevation remained but the anterolateral leads showed larger R wave voltages, more profound anterior ST depression, and lateral ST elevation (fig 2). Subsequent creatine kinase concentration was 4754 U/l and troponin T concentration was 28.03 ng/ml.
Figure 2.
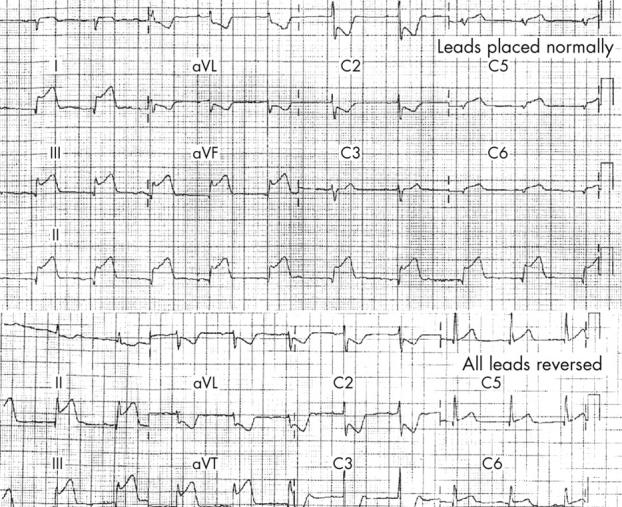
ECGs with leads placed normally (top) and with leads reversed.
The patient was thrombolysed with streptokinase but the ECG changes and symptoms persisted. Therefore, coronary angiography was undertaken through the right femoral arterial route.
The anatomical left coronary system (right sided) was engaged with a left Judkins 4 catheter and was visualised in the right anterior oblique projection. A severe proximal left anterior descending artery lesion was identified (fig 3). The anatomical right coronary artery (left sided) was engaged with a right Judkins 4 catheter but with a counter clockwise rotation. A significant lesion was shown proximally in the right coronary artery (fig 4).
Figure 3.

Coronary angiography showing a severe lesion (arrow) in the left anterior descending artery (equivalent left anterior oblique (LAO) cranial view).
Figure 4.

Coronary angiography showing a severe lesion (arrow) in the right coronary artery (equivalent LAO view).
On the basis of the acute ECG findings the anatomical right coronary artery stenosis was presumed to be the culprit lesion and was stented with a 3.5 × 18 mm AVE stent. However, the hyperacute ST changes did not resolve and the arterial pressures did not improve. It was also apparent that during left coronary injection the inferior ST segments rose transiently. Therefore, the left anterior descending artery was directly stented with 3.0 × 15 mm AVE stent, with a good angiographic result (fig 5).
Figure 5.

Angiographic result of direct stenting to the left anterior descending artery.
There was immediate improvement in the patient’s symptoms and arterial pressures with an associated resolution of the inferolateral ECG changes. Echocardiography after the intervention showed well preserved left ventricular function with no wall motion abnormality.
DISCUSSION
Ischaemic heart disease occurs rarely in dextrocardia because the anatomical abnormality is uncommon.1 These patients share the same risk as the general population for ischaemic heart disease.
This case is of interest for several reasons. Firstly, we have shown that it is possible to successfully engage the coronary arteries with standard catheters, if the position of the aorta is also reversed, as has previously been reported.2 Secondly, the position of the x ray image intensifier relative to the patient was maintained as the mirror image of normal practice, so that the images acquired also appeared as mirror images of the norm. This allowed normal manipulation of standard catheters.
Another unusual feature of this case is the non-resolution of the inferior ECG changes and haemodynamic abnormalities despite reperfusion of the vessel that conventionally supplies the inferior myocardium. One possible explanation is that the right coronary lesion was chronic and that an interruption of a collateral supply from the left system provoked the inferior changes. However, there was no evidence of any collateral circulation on coronary angiography. Another possible explanation is that this patient had an abnormal electrocardiographic response to myocardial injury because of abnormal depolarisation–repolarisation patterns secondary to situs inversus (the mirror image of normal visceral arrangement). To the best of our knowledge, there have been no similar reported cases. However, there is some evidence that situs inversus can be associated with abnormal development of the neural axis3 and so it is possible that there is an association with the neuromuscular development of the heart. These findings also suggest that ST changes on the ECG may be secondary to an abnormal response to ischaemia in patients with dextrocardia.
REFERENCES
- 1.Rosenburg HN, Rosenbuerg IN. Simultaneous association of situs inversus, coronary artery disease and hiatus hernia. Ann Intern Med 1949;30:851–9. [DOI] [PubMed] [Google Scholar]
- 2.Robinson N, Golledge P, Timmis A. Coronary stent deployment in situs inversus. Heart 2001;86:e15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tubbs RS, Wellons JC 3rd, Salter G, et al. ntracranial anatomic asymmetry in situs inversus totalis. Anat Embryol 2003;206:199–202. [DOI] [PubMed] [Google Scholar]