

Abstract
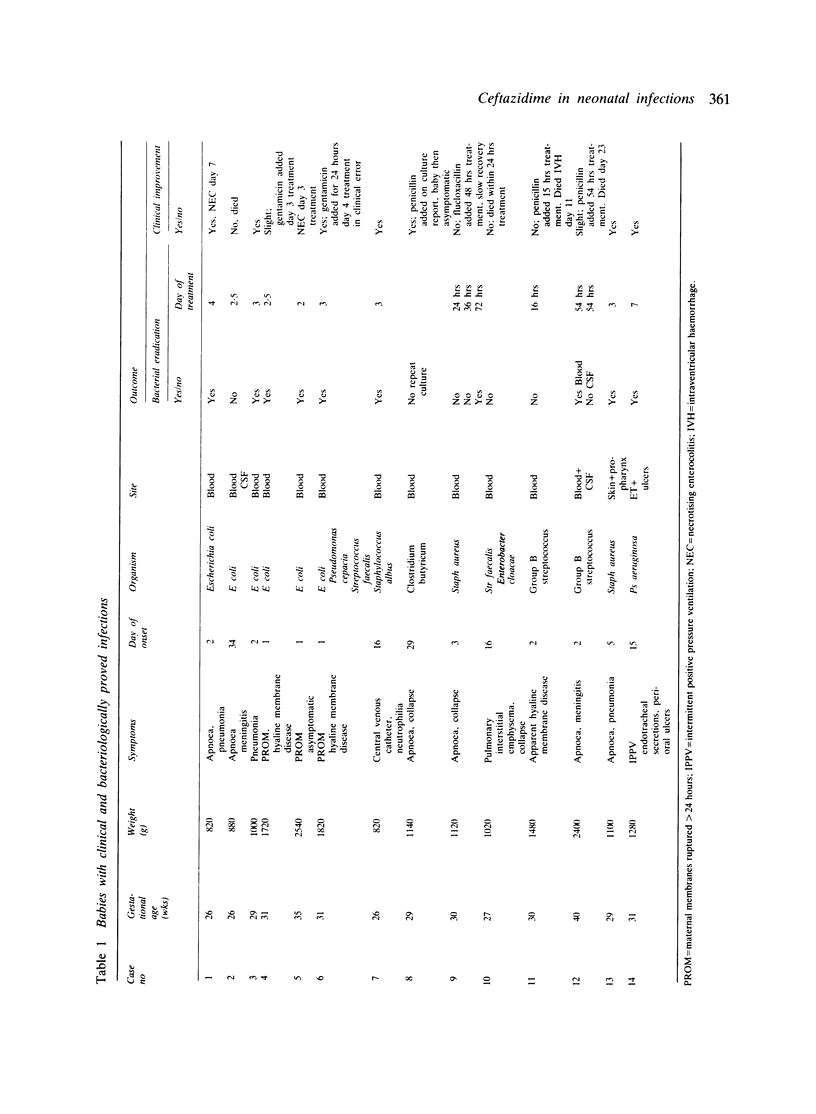
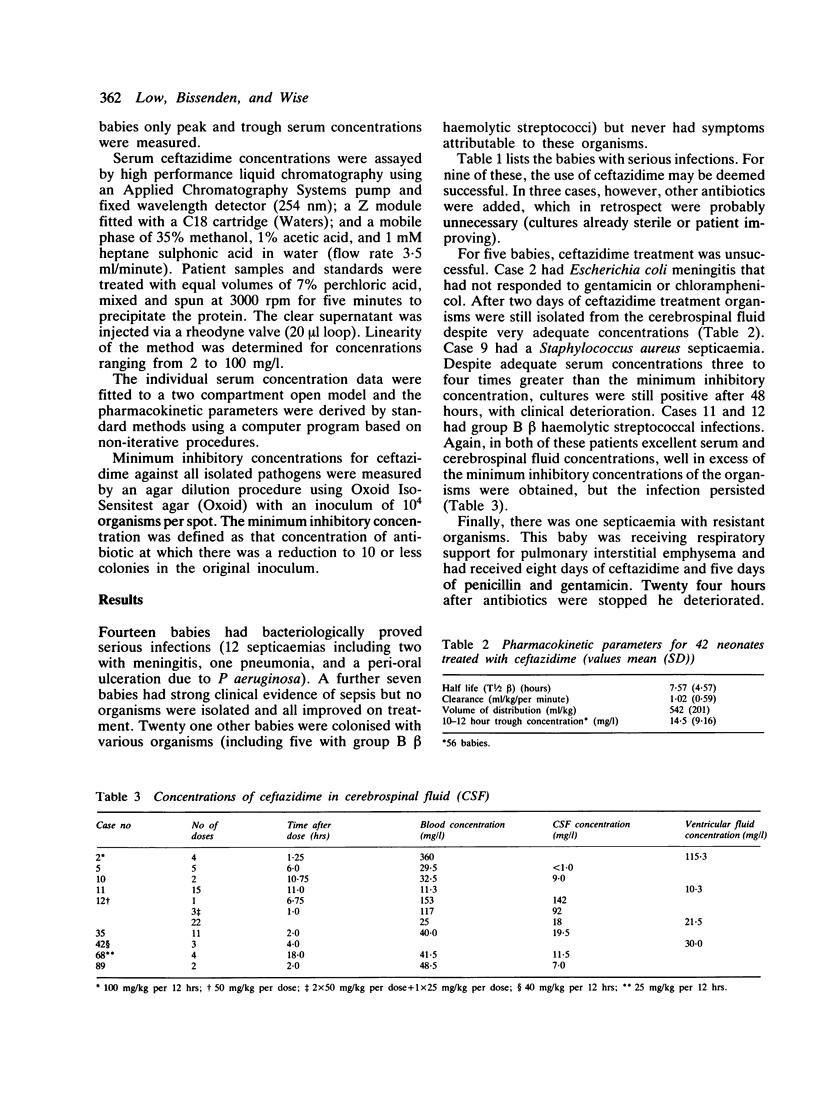
Ninety one neonates received 108 courses of intravenous ceftazidime (25 mg/kg, 12 hourly) over a study period of 15 months. Fourteen had clinically and bacteriologically proved infections. Only one of these had resistant organisms. Four (two with group B beta haemolytic streptococcal infections, one with Escherichia coli meningitis, and one with Staphylococcal aureus septicaemia) failed to respond despite adequate treatment. Bacteriological eradication or clinical improvement, or both, were obtained in the remaining nine. Routine biochemical and haematological values were monitored and there were no side effects. High serum ceftazidime concentrations, well exceeding the minimum inhibitory concentration for most common neonatal pathogens were obtained and maintained throughout treatment. Penetration into the cerebrospinal fluid was excellent in eight of the nine cases studied. Ceftazidime has a theoretical role as a broad spectrum antibiotic suitable for neonatal use with no evident side effects. In this study, however, it was only appropriate for Gram negative infections, and was ineffective against Gram positive organisms. Ceftazidime cannot therefore be recommended as monotherapy before the results of bacteriological culture are known.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Chang M. J., Escobedo M., Anderson D. C., Hillman L., Feigin R. D. Kanamycin and gentamicin treatment of neonatal sepsis and meningitis. Pediatrics. 1975 Nov;56(5):695–699. [PubMed] [Google Scholar]
- Deveikis A., Schauf V., Mizen M., Riff L. Antimicrobial therapy of experimental group B streptococcal infection in mice. Antimicrob Agents Chemother. 1977 May;11(5):817–820. doi: 10.1128/aac.11.5.817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elfving J., Pettay O., Raivio M. A follow-up study on the cochlear, vestibular and renal function in children treated with gentamicin in the newborn period. Chemotherapy. 1973;18(3):141–153. doi: 10.1159/000221256. [DOI] [PubMed] [Google Scholar]
- Feldman W. E. Concentrations of bacteria in cerebrospinal fluid of patients with bacterial meningitis. J Pediatr. 1976 Apr;88(4 Pt 1):549–552. doi: 10.1016/s0022-3476(76)80003-0. [DOI] [PubMed] [Google Scholar]
- Itsarayoungyuen S., Riff L., Schauf V., Hamilton L., Otrembiak J., Vidyasagar D. Tobramycin and gentamicin are equally safe for neonates: results of a double-blind randomized trial with quantitative assessment of renal function. Pediatr Pharmacol (New York) 1982;2(2):143–155. [PubMed] [Google Scholar]
- Kafetzis D. A., Brater D. C., Kapiki A. N., Papas C. V., Dellagrammaticas H., Papadatos C. J. Treatment of severe neonatal infections with cefotaxime. Efficacy and pharmacokinetics. J Pediatr. 1982 Mar;100(3):483–489. doi: 10.1016/s0022-3476(82)80466-6. [DOI] [PubMed] [Google Scholar]
- Kim K. S., Anthony B. F. Penicillin tolerance in group B streptococci isolated from infected neonates. J Infect Dis. 1981 Nov;144(5):411–419. doi: 10.1093/infdis/144.5.411. [DOI] [PubMed] [Google Scholar]
- Mulhall A., de Louvois J., Hurley R. Incidence of potentially toxic concentrations of gentamicin in the neonate. Arch Dis Child. 1983 Nov;58(11):897–900. doi: 10.1136/adc.58.11.897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Placzek M., Whitelaw A., Want S., Sahathevan M., Darrell J. Piperacillin in early neonatal infection. Arch Dis Child. 1983 Dec;58(12):1006–1009. doi: 10.1136/adc.58.12.1006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaad U. B., McCracken G. H., Jr, Threlkeld N., Thomas M. L. Clinical evaluation of a new broad-spectrum oxa-beta-lactam antibiotic, moxalactam, in neonates and infants. J Pediatr. 1981 Jan;98(1):129–136. doi: 10.1016/s0022-3476(81)80559-8. [DOI] [PubMed] [Google Scholar]
- Schauf V., Deveikis A., Riff L., Serota A. Antibiotic-killing kinetics of group B streptococci. J Pediatr. 1976 Aug;89(2):194–198. doi: 10.1016/s0022-3476(76)80446-5. [DOI] [PubMed] [Google Scholar]
- Snelling S., Hart C. A., Cooke R. W. Ceftazidime or gentamicin plus benzylpenicillin in neonates less than forty-eight hours old. J Antimicrob Chemother. 1983 Jul;12 (Suppl A):353–356. doi: 10.1093/jac/12.suppl_a.353. [DOI] [PubMed] [Google Scholar]
- Summary of the workshop on perinatal infections due to group B Streptococcus. J Infect Dis. 1977 Jul;136(1):137–152. doi: 10.1093/infdis/136.1.137. [DOI] [PubMed] [Google Scholar]
- Walstad R. A., Hellum K. B., Blika S., Dale L. G., Fredriksen T., Myhre K. I., Spencer G. R. Pharmacokinetics and tissue penetration of ceftazidime: studies on lymph, aqueous humour, skin blister, cerebrospinal and pleural fluid. J Antimicrob Chemother. 1983 Jul;12 (Suppl A):275–282. doi: 10.1093/jac/12.suppl_a.275. [DOI] [PubMed] [Google Scholar]
- Yamauchi T., Hill D. E., Steele R. W. The use of ceftizoxime in neonates. J Antimicrob Chemother. 1982 Nov;10 (Suppl 100):297–301. doi: 10.1093/jac/10.suppl_c.297. [DOI] [PubMed] [Google Scholar]
- de Louvois J., James J., Mulhall A. Latamoxef and the newborn. Arch Dis Child. 1984 Apr;59(4):346–350. doi: 10.1136/adc.59.4.346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Louvois J., Mulhall A., Hurley R. Cefuroxime in the treatment of neonates. Arch Dis Child. 1982 Jan;57(1):59–62. [PMC free article] [PubMed] [Google Scholar]