

Abstract
From January 1963 to December 1965 inclusive 192 men with duodenal ulcer were treated by elective truncal vagotomy and pyloroplasty with one death. Ten subsequent deaths were due to causes unrelated to the ulcer or operation, and 17 patients became untraceable. The remaining 164 patients have been followed up for five to eight years. The late results have been compared with those obtained in a previous study of patients five to eight years after truncal vagotomy and gastroenterostomy, truncal vagotomy and antrectomy, and subtotal gastrectomy respectively for duodenal ulcer.
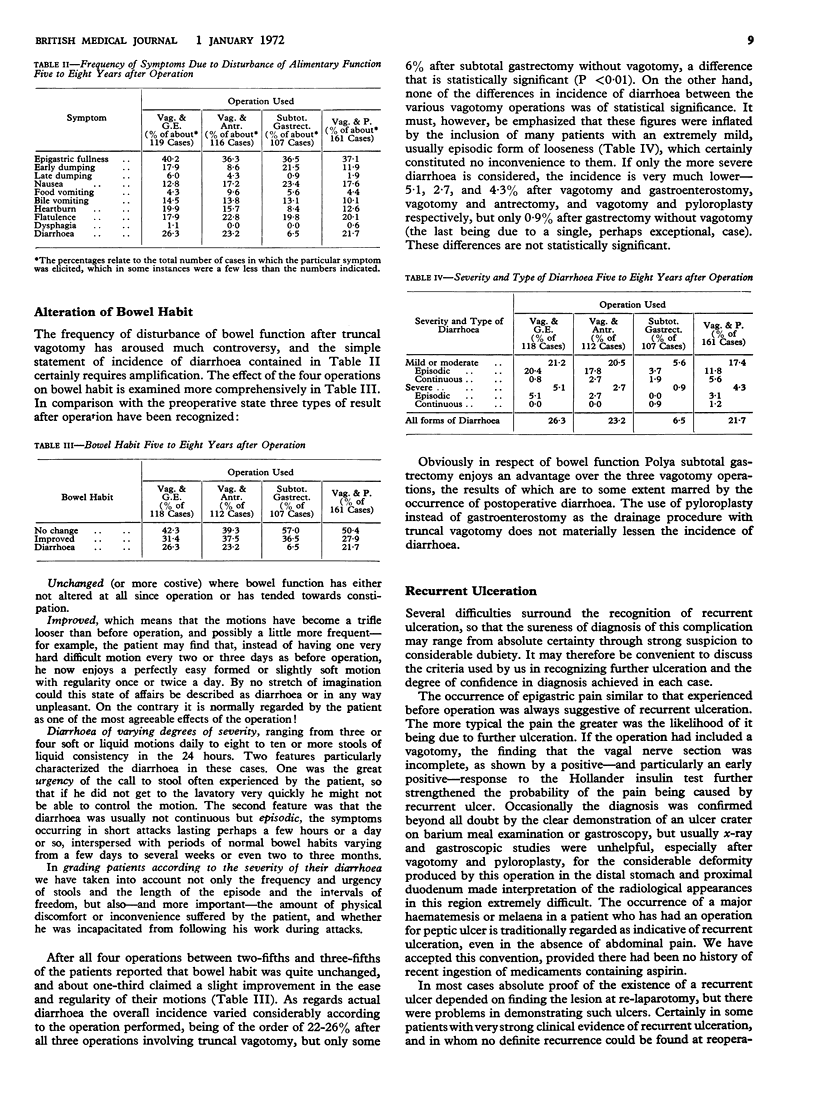
Of the various postgastric operation syndromes early dumping, late dumping, bilious vomiting, and diarrhoea were all less frequent, but not significantly so, after vagotomy and pyloroplasty than after vagotomy and gastroenterostomy.
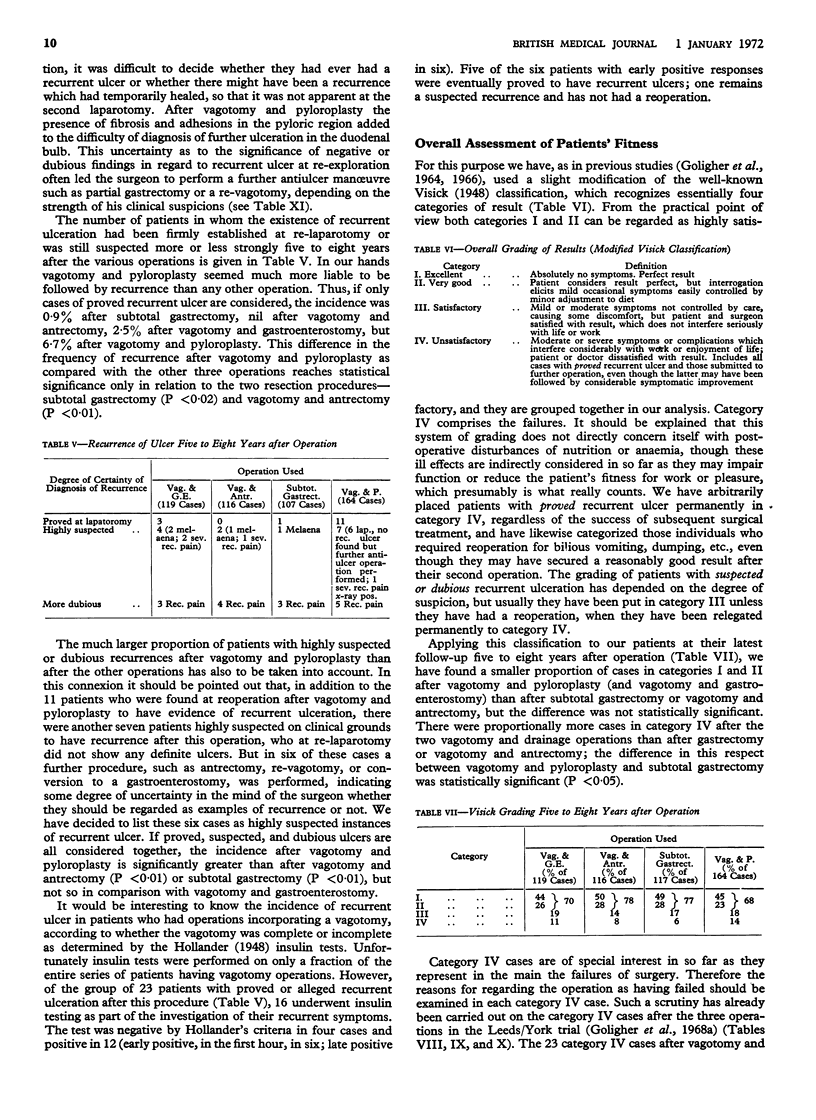
Recurrent ulceration was commoner after vagotomy and pyloroplasty than after all the other operations, the incidence of proved and suspected recurrent ulcers being respectively 6·7 and 7·3% after vagotomy and pyloroplasty, but only 2·5 and 5·9% after vagotomy and gastroenterostomy, 0 and 5·2% after vagotomy and antrectomy, and 0·9 and 3·7% after subtotal gastrectomy. The differences between vagotomy and pyloroplasty and vagotomy and antrectomy or subtotal gastrectomy are statistically significant, but those between vagotomy and pyloroplasty and vagotomy and gastroenterostomy are not.
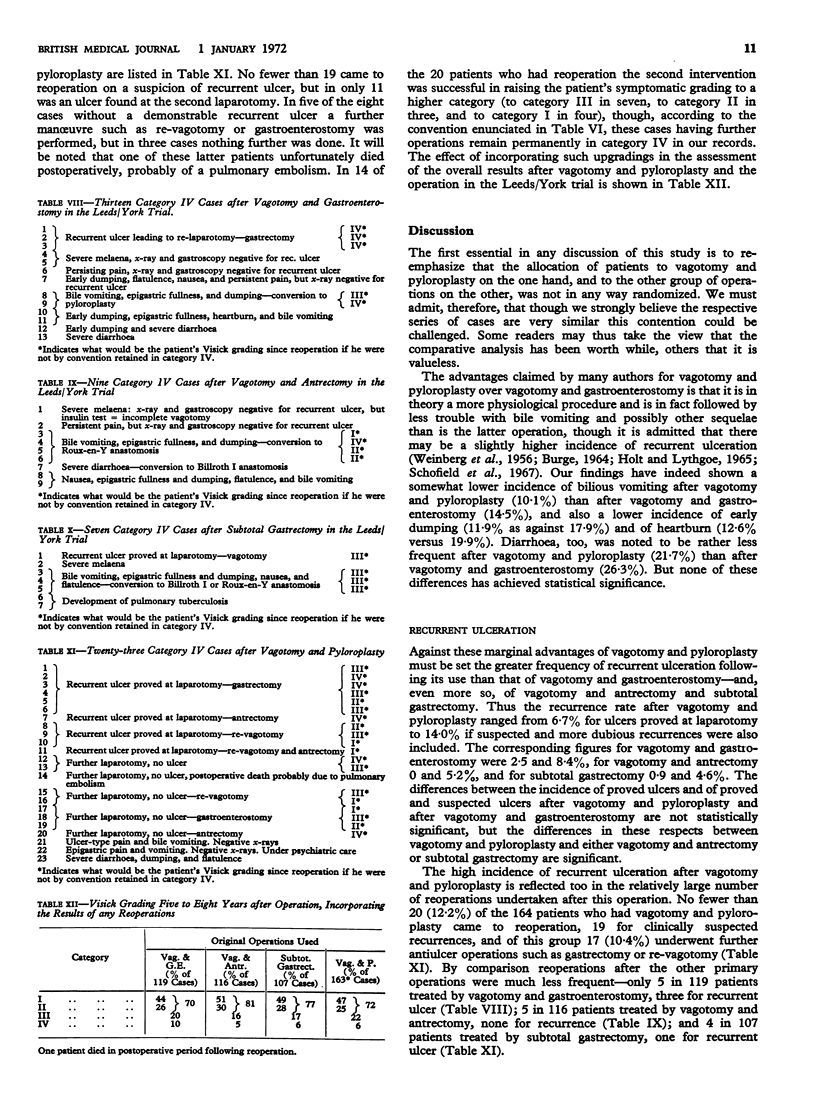
Overall assessment (Visick grading) of the outcome gave poorer results after vagotomy and pyloroplasty than after any other operation, with 14% of category IV cases after vagotomy and pyloroplasty, 11% after vagotomy and gastroenterostomy, 8% after vagotomy and antrectomy, and 6% after subtotal gastrectomy—differences that are significant between vagotomy and pyloroplasty and vagotomy and antrectomy or subtotal gastrectomy but not between vagotomy and pyloroplasty and vagotomy and gastroenterostomy.
In the light of these findings it is suggested that truncal vagotomy and pyloroplasty has not lived up to expectations and its place as the currently most popular procedure in the elective surgical treatment of duodenal ulcer should be reconsidered.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Amdrup E., Jensen H. E. Selective vagotomy of the parietal cell mass preserving innervation of the undrained antrum. A preliminary report of results in patients with duodenal ulcer. Gastroenterology. 1970 Oct;59(4):522–527. [PubMed] [Google Scholar]
- CLARK C. G., MURRAY J. G. The Burge test for complete vagotomy. J R Coll Surg Edinb. 1963 Apr;8:212–218. [PubMed] [Google Scholar]
- Cox A. G., Cooke W. M. Vagotomy for peptic ulcer. Br Med J. 1970 Feb 14;1(5693):432–433. doi: 10.1136/bmj.1.5693.432-c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fawcett A. N., Johnston D., Duthie H. L. Revagotomy for recurrent ulcer after vagotomy and drainage for duodenal ulcer. Br J Surg. 1969 Feb;56(2):111–116. doi: 10.1002/bjs.1800560208. [DOI] [PubMed] [Google Scholar]
- Frimer M. L., Cohen M. M., Harrison R. C., Holubitsky I. B. The selective nerve stain leucomethylene blue as an intraoperative aid to achieving complete vagotomy. Gut. 1970 Oct;11(10):881–882. doi: 10.1136/gut.11.10.881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GOLIGHER J. C., PULVERTAFT C. N., WATKINSON G. CONTROLLED TRIAL OF VAGOTOMY AND GASTRO- ENTEROSTOMY, VAGOTOMY AND ANTRECTOMY, AND SUBTOTAL GASTRECTOMY IN ELECTIVE TREATMENT OF DUODENAL ULCER: INTERIM REPORT. Br Med J. 1964 Feb 22;1(5381):455–460. doi: 10.1136/bmj.1.5381.455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillespie G., Elder J. B., Gillespie I. E., Kay A. W., Campbell E. H. The long term stability of the insulin test. Gastroenterology. 1970 May;58(5):625–632. [PubMed] [Google Scholar]
- Goligher J. C., Pulvertaft C. N., De Dombal F. T., Clark C. G., Conyers J. H., Duthie H. L., Feather D. B., Latchmore A. J., Matheson T. S., Shoesmith J. H. Clinical comparison of vagotomy and pyloroplasty with other forms of elective surgery for duodenal ulcer. Br Med J. 1968 Jun 29;2(5608):787–789. doi: 10.1136/bmj.2.5608.787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goligher J. C., Pulvertaft C. N., De Dombal F. T., Conyers J. H., Duthie H. L., Feather D. B., Latchmore A. J., Shoesmith J. H., Smiddy F. G., Willson-Pepper J. Five to eight-year results of Leeds-York controlled trial of elective surgery for duodenal ulcer. Br Med J. 1968 Jun 29;2(5608):781–787. doi: 10.1136/bmj.2.5608.781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grassi G. A new test for complete nerve section during vagotomy. Br J Surg. 1971 Mar;58(3):187–189. doi: 10.1002/bjs.1800580309. [DOI] [PubMed] [Google Scholar]
- HOLT R. L., LYTHGOE J. P. THE TREATMENT OF CHRONIC DUODENAL ULCER BY VAGOTOMY AND ANTERIOR PYLORECTOMY. Br J Surg. 1965 Jan;52:27–32. doi: 10.1002/bjs.1800520107. [DOI] [PubMed] [Google Scholar]
- Holle F. 34. Physiologische Operationen in der Ulcuschirurgie. Langenbecks Arch Chir. 1967;319:233–237. doi: 10.1007/BF02659265. [DOI] [PubMed] [Google Scholar]
- Johnston D., Thomas D. G., Checketts R. G., Duthie H. L. An assessment of postoperative testing for completeness of vagotomy. Br J Surg. 1967 Oct;54(10):831–833. doi: 10.1002/bjs.1800541006. [DOI] [PubMed] [Google Scholar]
- Johnston D., Wilkinson A. R. Highly selective vagotomy without a drainage procedure in the treatment of duodenal ulcer. Br J Surg. 1970 Apr;57(4):289–296. doi: 10.1002/bjs.1800570414. [DOI] [PubMed] [Google Scholar]
- Jordan P. H., Jr, Condon R. E. A prospective evaluation of vagotomy-pyloroplasty and vagotomy-antrectomy for treatment of duodenal ulcer. Ann Surg. 1970 Oct;172(4):547–563. doi: 10.1097/00000658-197010000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kennedy T., Connell A. M. Selective or truncal vagotomy? A double-blind randomised controlled trial. Lancet. 1969 May 3;1(7601):899–901. doi: 10.1016/s0140-6736(69)92541-0. [DOI] [PubMed] [Google Scholar]
- Kennedy T., Connell A. M. Selective or truncal vagotomy? Lancet. 1970 Mar 28;1(7648):675–675. doi: 10.1016/s0140-6736(70)90908-6. [DOI] [PubMed] [Google Scholar]
- Kronborg O., Malmström J., Christiansen P. M. A comparison between the results of truncal and selective vagotomy in patients with duodenal ulcer. Scand J Gastroenterol. 1970;5(6):519–524. [PubMed] [Google Scholar]
- Lee M. A selective stain to detect the vagus nerve in the operation of vagotomy. Br J Surg. 1969 Jan;56(1):10–13. doi: 10.1002/bjs.1800560104. [DOI] [PubMed] [Google Scholar]
- Mason M. C., Giles G. R. The postoperative insulin test--a further assessment. Br J Surg. 1969 May;56(5):384–384. [PubMed] [Google Scholar]
- Mason M. C., Giles G. R. The postoperative insulin test: failure to detect incomplete vagotomy in patients with high acid levels. Br J Surg. 1968 Nov;55(11):865–865. [PubMed] [Google Scholar]
- Schofield P. F., Watson-Williams E. J., Sorrell V. F. Vagotomy and pyloric drainage for chronic duodenal ulcer. Long-term results. Arch Surg. 1967 Oct;95(4):615–624. doi: 10.1001/archsurg.1967.01330160085011. [DOI] [PubMed] [Google Scholar]
- WEINBERG J. A., STEMPIEN S. J., MOVIUS H. J., DAGRADI A. E. Vagotomy and pyloroplasty in the treatment of duodenal ulcer. Am J Surg. 1956 Aug;92(2):202–207. doi: 10.1016/s0002-9610(56)80060-3. [DOI] [PubMed] [Google Scholar]