

Abstract
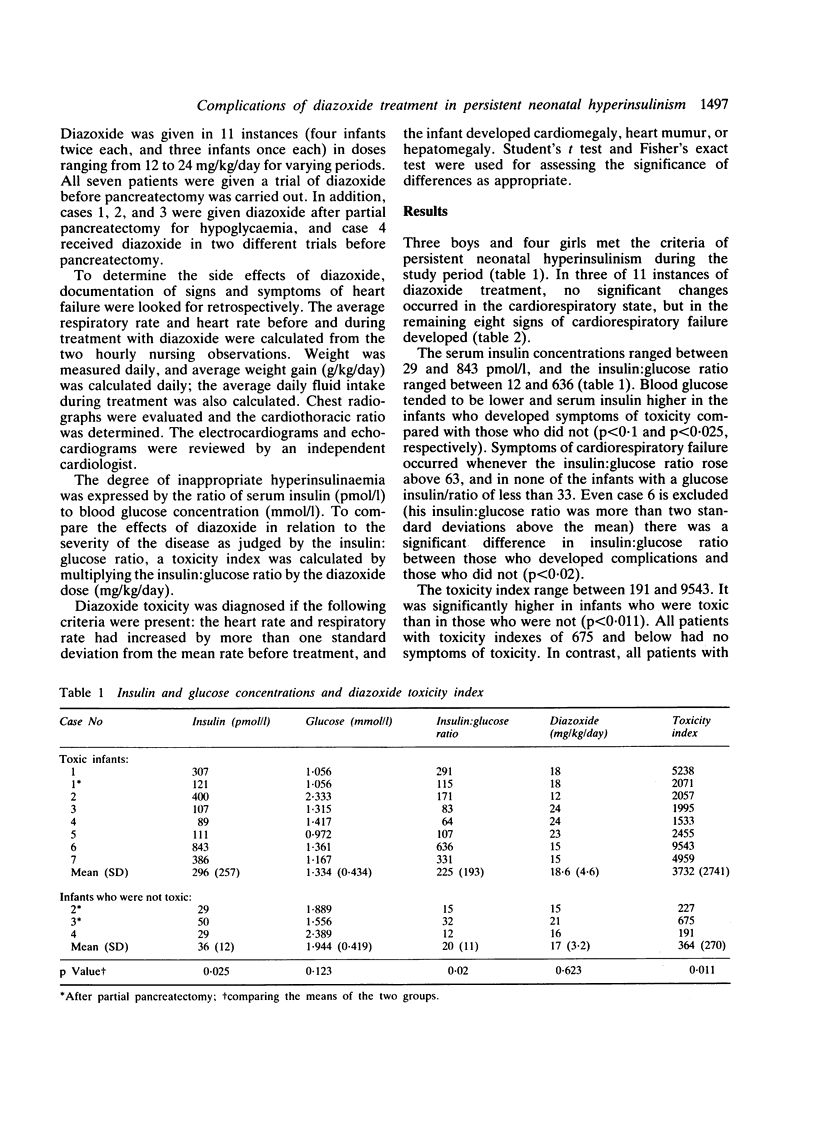
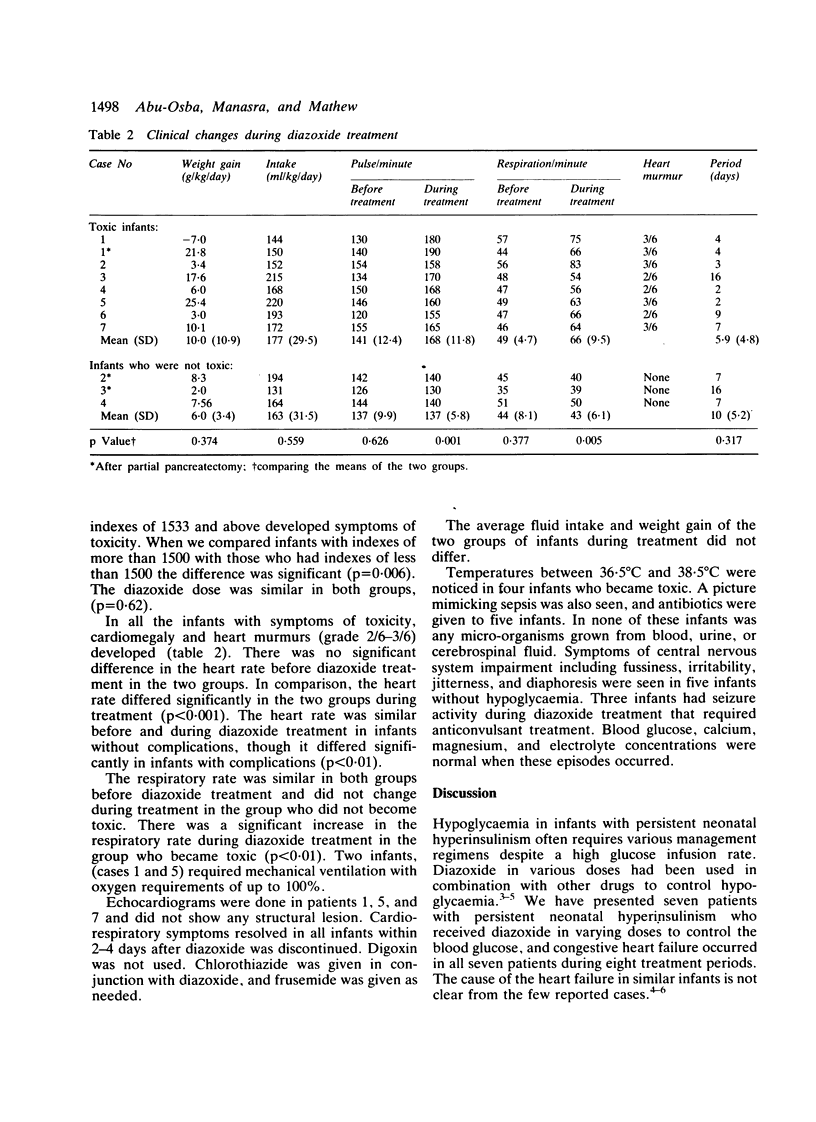
Seven infants with persistent neonatal hyperinsulinism were treated in Dhahran Health Centre from 1983 to 1986. The insulin:glucose ratio (serum insulin concentration pmol/l) divided by the blood glucose concentration (mmol/l) ranged from 12 to 636, mean (SD) 177 (201). To control hypoglycaemia, diazoxide (12-24 mg/kg/day) was given in a continuous intravenous glucose infusion (12-22 mg/kg/min) on 11 separate occasions, four infants twice each and three infants once each. An increase of more than one standard deviation in the heart and respiratory rates, together with other symptoms of heart failure, was considered to be evidence of diazoxide toxicity. Cardiorespiratory failure (toxicity) occurred on eight of the 11 occasions (73%) in seven infants. The average daily fluid intake, weight change, respiratory rate and heart rate before treatment were similar whether or not the infant developed toxicity. A diazoxide toxicity index was obtained by multiplying the dose of diazoxide by the insulin:glucose ratio to relate the diazoxide dose to the severity of the disease. In all instances when the toxicity index was more than 1533 (mean (SD) 3732 (2741) cardiac toxicity developed. In contrast, infants with a toxicity index of less than 675 (mean (SD) 364 (270), had no symptoms of toxicity. Symptoms were significantly related to the severity of the disease and the diazoxide dose. It is possible to use the toxicity index to predict the risk of toxicity and to calculate a safe dose of diazoxide in infants with persistent neonatal hyperinsulinism.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aynsley-Green A., Polak J. M., Bloom S. R., Gough M. H., Keeling J., Ashcroft S. J., Turner R. C., Baum J. D. Nesidioblastosis of the pancreas: definition of the syndrome and the management of the severe neonatal hyperinsulinaemic hypoglycaemia. Arch Dis Child. 1981 Jul;56(7):496–508. doi: 10.1136/adc.56.7.496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Breitweser J. A., Meyer R. A., Sperling M. A., Tsang R. C., Kaplan S. Cardiac septal hypertrophy in hyperinsulinemic infants. J Pediatr. 1980 Mar;96(3 Pt 2):535–539. doi: 10.1016/s0022-3476(80)80862-6. [DOI] [PubMed] [Google Scholar]
- Gillies D. R. Complications of diazoxide in the treatment of nesidioblastosis. Arch Dis Child. 1985 May;60(5):500–501. doi: 10.1136/adc.60.5.500-b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gutgesell H. P., Speer M. E., Rosenberg H. S. Characterization of the cardiomyopathy in infants of diabetic mothers. Circulation. 1980 Feb;61(2):441–450. doi: 10.1161/01.cir.61.2.441. [DOI] [PubMed] [Google Scholar]
- Heitz P. U., Klöppel G., Häcki W. H., Polak J. M., Pearse A. G. Nesidioblastosis: the pathologic basis of persistent hyperinsulinemic hypoglycemia in infants. Morphologic and quantitative analysis of seven cases based on specific immunostaining and electron microscopy. Diabetes. 1977 Jul;26(7):632–642. doi: 10.2337/diab.26.7.632. [DOI] [PubMed] [Google Scholar]
- Mathew P. M., Young J. M., Abu-Osba Y. K., Mulhern B. D., Hammoudi S., Hamdan J. A., Sa'di A. R. Persistent neonatal hyperinsulinism. Clin Pediatr (Phila) 1988 Mar;27(3):148–151. doi: 10.1177/000992288802700307. [DOI] [PubMed] [Google Scholar]
- McGraw M. E., Price D. A. Complications of diazoxide in the treatment of nesidioblastosis. Arch Dis Child. 1985 Jan;60(1):62–64. doi: 10.1136/adc.60.1.62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salinas E. D., Jr, Mangurten H. H., Roberts S. S., Simon W. H., Cornblath M. Functioning islet cell adenoma in the newborn. Report of a case with failure of diazoxide. Pediatrics. 1968 Mar;41(3):646–653. [PubMed] [Google Scholar]
- Yakovac W. C., Baker L., Hummeler K. Beta cell nesidioblastosis in idiopathic hypoglycemia of infancy. J Pediatr. 1971 Aug;79(2):226–231. doi: 10.1016/s0022-3476(71)80105-1. [DOI] [PubMed] [Google Scholar]