

The 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children have been prepared as a supplement to this issue of CMAJ (a summary of the guidelines is included in the polywrap of this issue, and the complete set of guidelines is available online at www.cmaj.ca/cgi/content/full/176/8/S1/DC1).1 A rigorous, evidence-based approach was used to develop recommendations to guide practitioners and interested individuals to reach optimal health care decisions related to the individual and public health issues associated with obesity.
Despite major advances in our fundamental knowledge and steady progress in the management of obesity, Canada and the rest of the world are witnessing an alarming increase in the prevalence of obesity and its related health consequences, with 59% of adult Canadians being overweight and 23% being obese.2 What is more disturbing is the rapid increase in childhood obesity rates and the early onset of metabolic complications that track into adulthood and may lead to a shortened life expectancy.3 Health professionals can expect in their clinical encounters an increasing number of overweight and obese people at all ages presenting with a variety of physical and mental health issues. To date, interventions at the individual and population levels, with the latter focused mainly on individual risk factors, have been ineffective for the most part. Hence, sweeping prevention and intervention strategies are required to slow, and hopefully reverse, the alarming increase in obesity prevalence.
Previous clinical practice guidelines on the assessment and management of obesity have been based in large part on consensus statements by expert panels.4–7 Moreover, most focused on individuals rather than on communities or the population as a whole. Recognizing these deficiencies, Obesity Canada — a not-for-profit organization founded in 1999 to improve the health of Canadians by decreasing the occurrence of obesity — convened a panel of experts to determine whether a comprehensive set of clinical practice guidelines could be developed to address not only the management but also the prevention of obesity in both adults and children. Members of the Steering Committee and Expert Panel unanimously agreed on an evidence-based approach that adhered to the principles espoused by the Appraisal of Guidelines Research & Evaluation (AGREE) Instrument to provide a framework for assessing the quality of clinical practice guidelines.8 Through the process of developing the guidelines, which began in the spring of 2004, members of the Steering Committee and Expert Panel identified major gaps in knowledge regarding obesity treatment and prevention. The final set of clinical practice guidelines in the supplement to this issue of CMAJ are the culmination of work by a large panel of experts across Canada who freely volunteered their time and effort. Each recommendation in the guidelines is based on a systematic review of the literature and reflects the consensus of the relevant members of the Expert Panel and members of the Steering Committee. The recommendations have been graded based on the strength of the supporting evidence and in consideration of the harm and costs of the intervention, and its importance and value to the individual and population.
Ideally, clinical practice guidelines would inspire confidence by its users if they were developed with the necessary financial support to ensure the highest quality. Unfortunately, there is currently a lack of public funding for the development of practice guidelines in Canada. Therefore, funding was sought through sponsorships from pharmaceutical and food industry partners as well as through in-kind donations from nongovernmental organizations. The corporate sponsors were not involved in and had no influence on the development of the guidelines, the interpretation of the literature, the decision to publish or any aspect of publication of the guidelines. The arm's-length grants-in-aid solicited were managed in part by a third-party organization, independent of Obesity Canada, and were used to defray administrative and travel expenses incurred by members of the Steering Committee and Expert Panel to attend meetings and conference calls, and to defray publication, implementation and dissemination costs. None of the members of these committees received financial or in-kind remuneration for their contributions, other than reprint copies of the executive summary of the clinical practice guidelines.
What are the objectives of the guidelines?
The specific objectives of the guidelines were to establish a process for developing evidence-based recommendations to guide the management and prevention of obesity at the individual and population levels, to identify gaps in knowledge and care, to disseminate the information to a broad spectrum of health care providers, to assist in public health policy development and to inform an agenda for future research to improve the standards of care.
Who will benefit from the guidelines?
A broad range of populations, encompassing all age groups and population subgroups, are addressed by the clinical practice guidelines. The guidelines are directed at primary care and specialist health professionals working with overweight and obese adults and children in primary, secondary and tertiary care settings, as well as health policy-makers, government agencies at all levels, corporate and private sectors, and the public at large to bring about changes in the environment that are more conducive to healthy living. They may also assist individuals to make informed lifestyle choices.
What are the key recommendations?
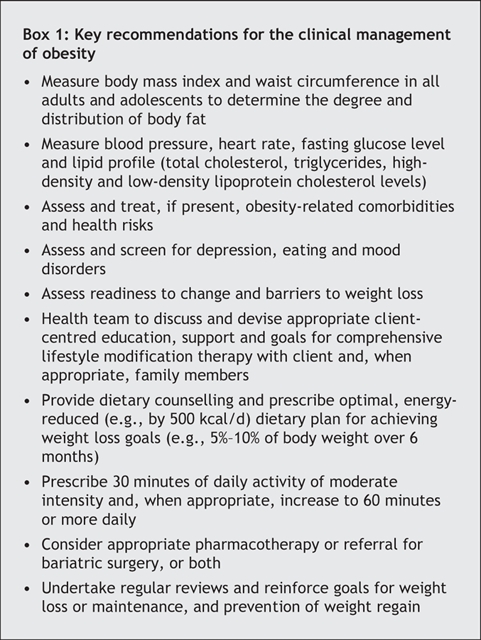
The full document contains an executive summary,1 which highlights the rationale, objectives, formulation and grading of the evidence-based recommendations, as well as all of the recommendations, which appear at the end of each of the 26 chapters. Obesity is a complex chronic disease that requires long-term and sustainable management strategies aimed at changing lifestyle habits and introducing healthier behaviours. Although the guidelines are not intended as a primer, they provide a stepwise client-centred approach to obesity management and prevention (Fig. 1). By simplifying the assessment and management strategies, health professionals will be better able to manage and prevent obesity in daily practice. Box 1 outlines the key recommendations for the assessment and stepwise approach to the management of obesity in adults.
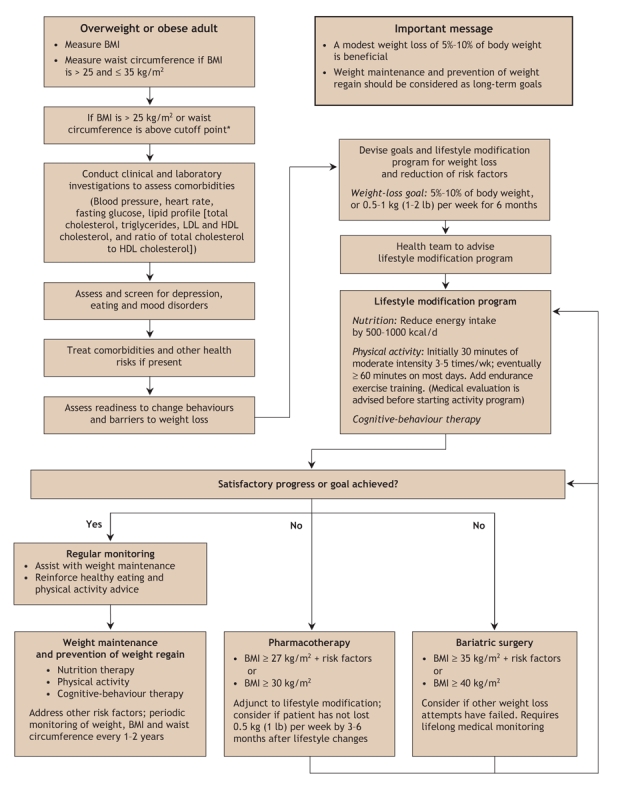
Fig. 1: Algorithm for the assessment and stepwise management of the overweight or obese adult. LDL = low-density lipoprotein, HDL = high-density lipoprotein. *Body mass index (BMI) and waist circumference cutoff points are different for some ethnic groups.
Box 1.
Canada was one of the first countries to adopt body mass index (BMI) as a useful surrogate anthropometric measure of adiposity. The 2003 guide to healthy body weight in adults realigned the Canadian classification of overweight and obesity with those of the World Health Organization and International Obesity Taskforce and classifies overweight and obesity based on BMI. In addition to BMI, we recognize within these guidelines the importance of body fat distribution as a strong predictor of the obesity-related health risks, notably type 2 diabetes, atherogenic dyslipidemia, hypertension and cardiovascular disease. We now recommend waist circumference measurement in all adults and adolescents as a new vital sign and an integral component of client assessment for global cardiometabolic risks. Specific cutoff points for different ethnic backgrounds, as recommended by the International Diabetes Federation, will be used to assess heath risks and determine intensity of management.
We recommend an assessment to determine the client's readiness to change behaviours, to identify barriers to weight loss and to screen for depression, eating and psychiatric disorders, in order to assist health professionals in successfully guiding their clients to initiate changes in lifestyle habits. Our recommendations also emphasize the role of a multidisciplinary health team and the importance of working together to create a nonjudgmental atmosphere that will ease the stigma and the feelings of blame and guilt experienced by many overweight and obese individuals. Developing an individualized, client-centred, comprehensive lifestyle modification program can help overweight and obese individuals achieve realistic weight loss or weight maintenance goals. Specific recommendations on nutrition and dietary therapy, physical activity and exercise therapy for weight loss are described. Positive reinforcement of behavioural changes through ongoing support and cognitive-behaviour therapy, when available, is encouraged. The increasingly important role of adjunctive pharmacotherapy and bariatric surgery constitute some of the key recommendations of the evidence-based clinical practice guidelines. Our guidelines stress the health benefits that could be derived from a modest 5%–10% loss of body weight. Long-term weight management should shift the focus from induction of weight loss to weight maintenance and prevention of relapse.
Although the majority of the recommendations are directed at the management of obesity, we realize that population health approaches will probably be more effective in preventing and reducing the prevalence of obesity. We recommend that prevention efforts at the population level target all age groups and more specifically recommend decreasing "screen time" and increasing the opportunities for healthy active living within schools, workplaces, homes and communities. Finally, recommendations on the dissemination and implementation of clinical practice guidelines are vital if we are to succeed in improving the standards of care and achieving success in the management and prevention of obesity.
Summary
The 2006 Canadian clinical practice guidelines, when supported by a solid dissemination and implementation strategy, are the essential first steps to initiate successful changes in clinical practice on the management and prevention of a serious societal and public health problem that is reaching epidemic proportions. We hope the guidelines will be incorporated into daily clinical practice and form the basis of care maps and standards of care for overweight and obese individuals. We also hope that, by providing integrated clinical and public health recommendations, these guidelines will serve to remind us that obesity is a societal and public health issue that urgently requires a call to action. Ideally, these guidelines will reach out to the public at large and interested parties beyond the health sector, including policy-makers at various levels of government, to bring about changes in the environment that are more conducive to healthy living and activity practices and ultimately to reduce the occurrence of obesity. We need to reinstate physical activity into the daily lives of all Canadians to optimize our health status. A healthier population will transform us into a wealthier and more productive nation. The serious personal and societal consequences of inaction on the obesity epidemic can no longer be ignored.
@ See related article page 1109
Acknowledgments
I thank Drs. Denis Drouin and James Douketis for their help in formulating the algorithm.
Footnotes
Competing interests: David Lau owns common shares in GlaxoSmithKline and Eli Lilly. He is a consultant to Abbott Laboratories, Ltd., AstraZeneca Canada Inc., Merck Frosst Canada Inc., Bristol-Myers Squibb Canada, Eli Lilly Canada Inc., Oryx Pharmaceuticals Inc., Pfizer Canada Inc., sanofi-aventis Canada Inc., Servier Canada Inc. and Solvay Pharma Inc.; and has received speaker fees from Abbott Laboratories, Ltd., AstraZeneca Canada Inc., GlaxoSmithKline, Merck Frosst Canada Inc., Merck/Schering, Eli Lilly Canada Inc., sanofi-aventis Canada Inc. and Novo Nordisk Canada Inc.; research grants from AstraZeneca Canada Inc., Bristol Myers Squibb, Dainippon Pharmaceuticals, GlaxoSmithKline, Pfizer Canada Inc., and sanofi-aventis Canada Inc.; and travel assistance to attend international meetings from Abbott Laboratories, Ltd., AstraZeneca Canada Inc. and sanofi-aventis Canada Inc.
Correspondence to: Dr. David C.W. Lau, Departments of Medicine, Biochemistry and Molecular Biology, Julia McFarlane Diabetes Research Centre, Diabetes and Endocrine Research Group, University of Calgary, 2521–3330 Hospital Dr. NW, Calgary AB T2N 4N1; dcwlau@ucalgary.ca
REFERENCES
- 1.Lau DCW, Douketis JD, Morrison K, et al; Obesity Canada Clinical Practice Guidelines Expert Panel. 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children [summary]. CMAJ 2007;176(8 Suppl):S1-13. [For the complete set of guidelines, go to www.cmaj.ca/cgi/content/full/176/8/S1/DC1] [DOI] [PMC free article] [PubMed]
- 2.Tjepkema M. Measured obesity: adult obesity in Canada — measured height and weight. In: Nutrition: findings from the Canadian Community Health Survey. Ottawa: Statistics Canada; 2005. Issue no 1. Cat no 82-620-MWE2005001. Available: www.statcan.ca/english/research/82-620-MIE/2005001/pdf/aobesity.pdf (accessed 2007 Mar 5).
- 3.Shields M. Measured obesity: overweight Canadian children and adolescents. In: Nutrition: findings from the Canadian Community Health Survey. Ottawa: Statistics Canada; 2005. Issue no 1. Cat no 82-620-MWE2005001. Available: www.statcan.ca/english/research/82-620-MIE/2005001/pdf/cobesity.pdf (accessed 2007 Mar 5).
- 4.National Institutes of Health. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults — the evidence report. Obes Res 1998;6:51S-209S. [PubMed]
- 5.Australian National Health and Medical Research Council. Clinical practice guidelines for the management of overweight and obesity in children and adolescents. Canberra: The Council; 2003. Available: www.health.gov.au/internet/wcms/Publishing.nsf/Content/obesityguidelines-guidelines-children.htm/$FILE/children.pdf (accessed 2007 Mar 5).
- 6.Scottish Intercollegiate Guidelines Network (SIGN). Management of obesity in children and young people. A national clinical guideline. Edinburgh: SIGN; 2003. Available: www.sign.ac.uk/pdf/sign69.pdf (accessed 2007 Mar 5).
- 7.Obesity. the prevention, identification, assessment and management of overweight and obesity in adults and children. London (UK): National Institute for Health and Clinical Excellence; 2006. [PubMed]
- 8.Appraisal of Guidelines for Research & Evaluation (AGREE) Instrument. London (UK): St. George's Medical School; 2001. Available: www.agreecollaboration.org/pdf/agreeinstrumentfinal.pdf (accessed 2007 Mar 5).