

Abstract
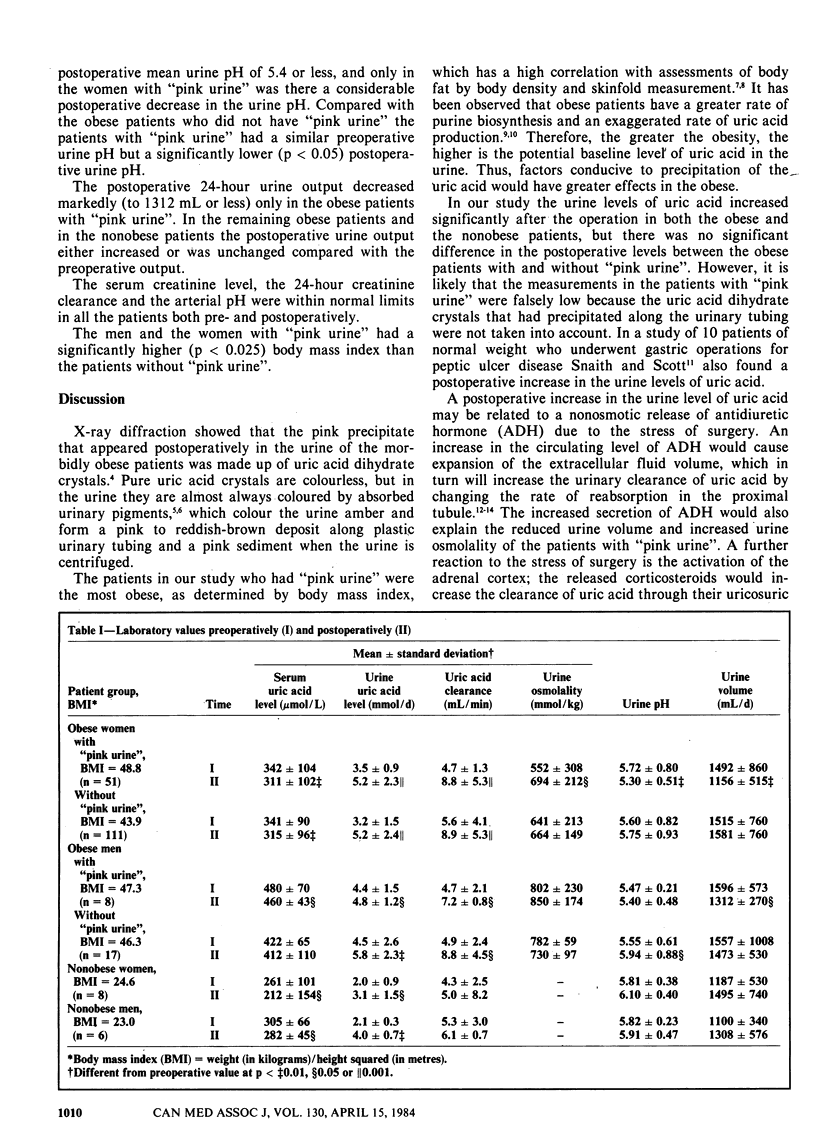
A pink coating on the inner surface of plastic urinary tubing, which gave the impression that the urine was pink, had frequently been noted 4 to 24 hours following gastric partitioning by means of a stapler in morbidly obese patients. A study was therefore done in 187 such patients as well as in 14 patients of normal weight who had undergone abdominal surgery of comparable magnitude. Postoperatively "pink urine" was observed in 32% of the obese patients but in none of the nonobese patients; however, a pink sediment remained following centrifugation of urine collected postoperatively from all the obese patients. Microscopy of this sediment showed crystals of uric acid dihydrate; these were infrequent in the preoperative specimens but present in high concentration in the postoperative specimens, particularly those of "pink urine". X-ray diffraction analysis confirmed the nature of the crystals. Preoperatively the obese patients had high-normal serum levels of uric acid. Postoperatively in all the groups of patients the serum levels of uric acid decreased while the urine levels and the urinary clearance of uric acid increased; the last two values, however, were significantly greater, both preoperatively and postoperatively, in those who were morbidly obese. Compared with the patients who did not have "pink urine" the patients with "pink urine" were significantly more obese and had a significantly lower postoperative urine pH. The latter also had a marked postoperative increase in urine osmolality and were the only patients to have a significant postoperative decrease in urine output. Thus, the pink colour of this group's urine was attributed to precipitation of uric acid crystals, fostered by a decrease in pH and an increase in concentration of the urine.
Full text
PDF
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Beck L. H. Clinical disorders of uric acid metabolism. Med Clin North Am. 1981 Mar;65(2):401–411. doi: 10.1016/s0025-7125(16)31531-0. [DOI] [PubMed] [Google Scholar]
- Cameron J. S., Simmonds H. A. Uric acid, gout and the kidney. J Clin Pathol. 1981 Nov;34(11):1245–1254. doi: 10.1136/jcp.34.11.1245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deitel M., Bojm M. A., Atin M. D., Zakhary G. S. Intestinal bypass and gastric partitioning for morbid obesity: a comparison. Can J Surg. 1982 May;25(3):283–289. [PubMed] [Google Scholar]
- Emmerson B. T. The effect of weight reduction on urate metabolism. Adv Exp Med Biol. 1974;41:429–433. doi: 10.1007/978-1-4757-1433-3_7. [DOI] [PubMed] [Google Scholar]
- HELMREICH M. L., JENKINS D., SWAN H. The adrenal cortical response to surgery. II. Changes in plasma and urinary corticosteroid levels in man. Surgery. 1957 Jun;41(6):895–909. [PubMed] [Google Scholar]
- HENNEMAN P. H., WALLACH S., DEMPSEY E. F. The metabolism defect responsible for uric acid stone formation. J Clin Invest. 1962 Mar;41:537–542. doi: 10.1172/JCI104507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keys A., Fidanza F., Karvonen M. J., Kimura N., Taylor H. L. Indices of relative weight and obesity. J Chronic Dis. 1972 Jul 1;25(6):329–343. doi: 10.1016/0021-9681(72)90027-6. [DOI] [PubMed] [Google Scholar]
- Mason E. E. Vertical banded gastroplasty for obesity. Arch Surg. 1982 May;117(5):701–706. doi: 10.1001/archsurg.1982.01380290147026. [DOI] [PubMed] [Google Scholar]
- Okada M., Takeshita M., Ueda K., Omae T., Hirota Y. Factors influencing the serum uric acid level. A study based on a population survey in Hisayama town, Kyushu, Japan. J Chronic Dis. 1980;33(10):607–612. doi: 10.1016/0021-9681(80)90003-x. [DOI] [PubMed] [Google Scholar]
- Rapoport A., Crassweller P. O., Husdan H., From G. L., Zweig M., Johnson M. D. The renal excretion of hydrogen ion in uric acid stone formers. Metabolism. 1967 Feb;16(2):176–188. doi: 10.1016/0026-0495(67)90110-2. [DOI] [PubMed] [Google Scholar]
- SANDBERG A. A., EIK-NES K., SAMUELS L. T., TYLER F. H. The effects of surgery on the blood levels and metabolism of 17-hydroxycorticosteroids in man. J Clin Invest. 1954 Nov;33(11):1509–1516. doi: 10.1172/JCI103029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snaith M. L., Scott J. T. Uric acid excretion and surgery. Ann Rheum Dis. 1972 May;31(3):162–165. doi: 10.1136/ard.31.3.162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Womersley J. A comparison of the skinfold method with extent of 'overweight' and various weight-height relationships in the assessment of obesity. Br J Nutr. 1977 Sep;38(2):271–284. doi: 10.1079/bjn19770088. [DOI] [PubMed] [Google Scholar]