

Abstract
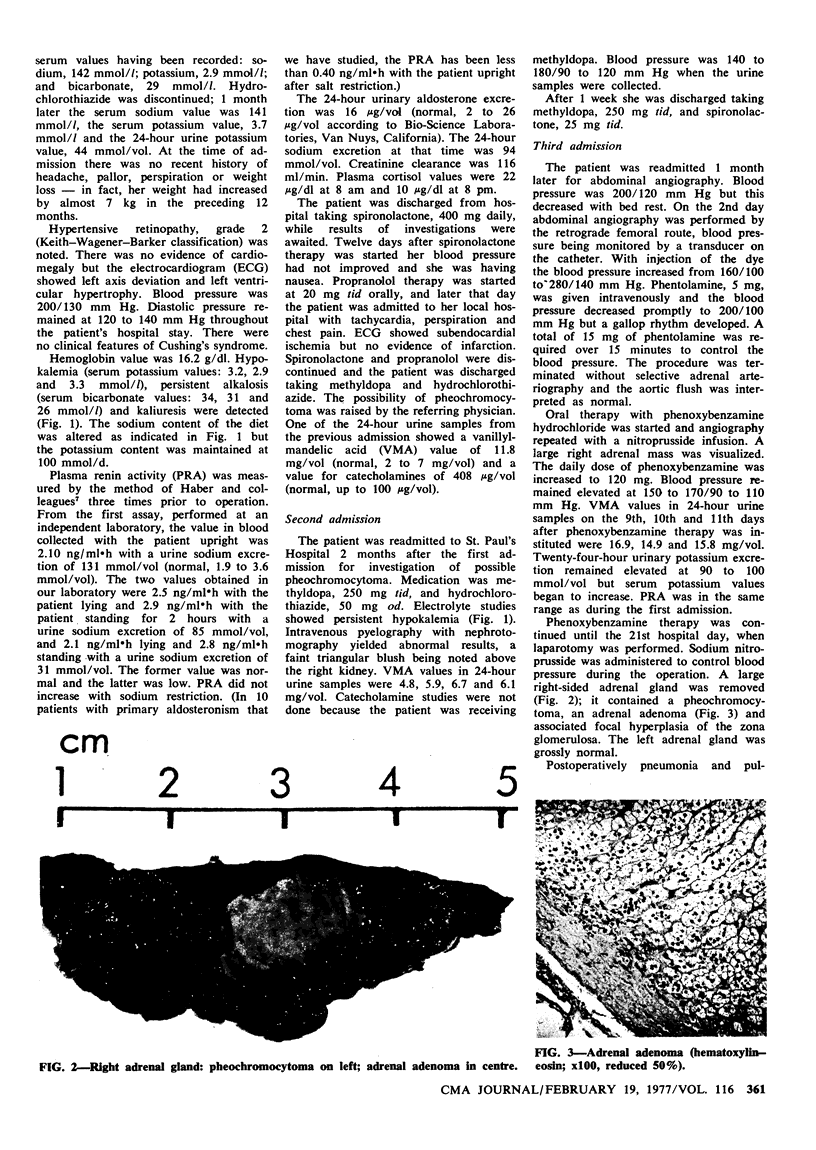
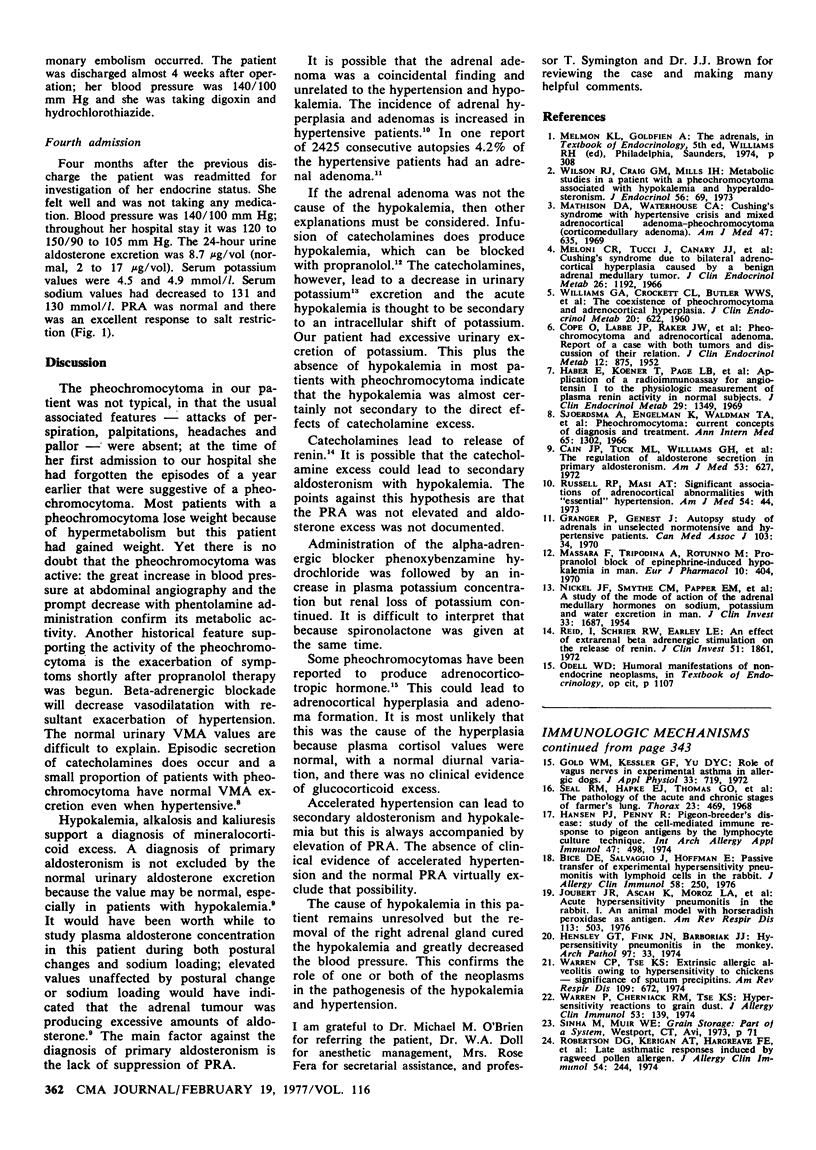
A 56-year-old woman had a 22-year history of hypertension. Investigation showed hypokalemia and kaliuresis without pronounced suppression of plasma renin activity or elevation of urinary aldosterone excretion. There was biochemical evidence of catecholamine metabolite excess but the usual clinical features of pheochromocytoma were absent. Laparotomy revealed a pheochromocytoma and adrenal adenoma in the right adrenal gland. Excision of the tumours was followed by resolution of the hypertension and metabolic abnormalities.
Full text
PDF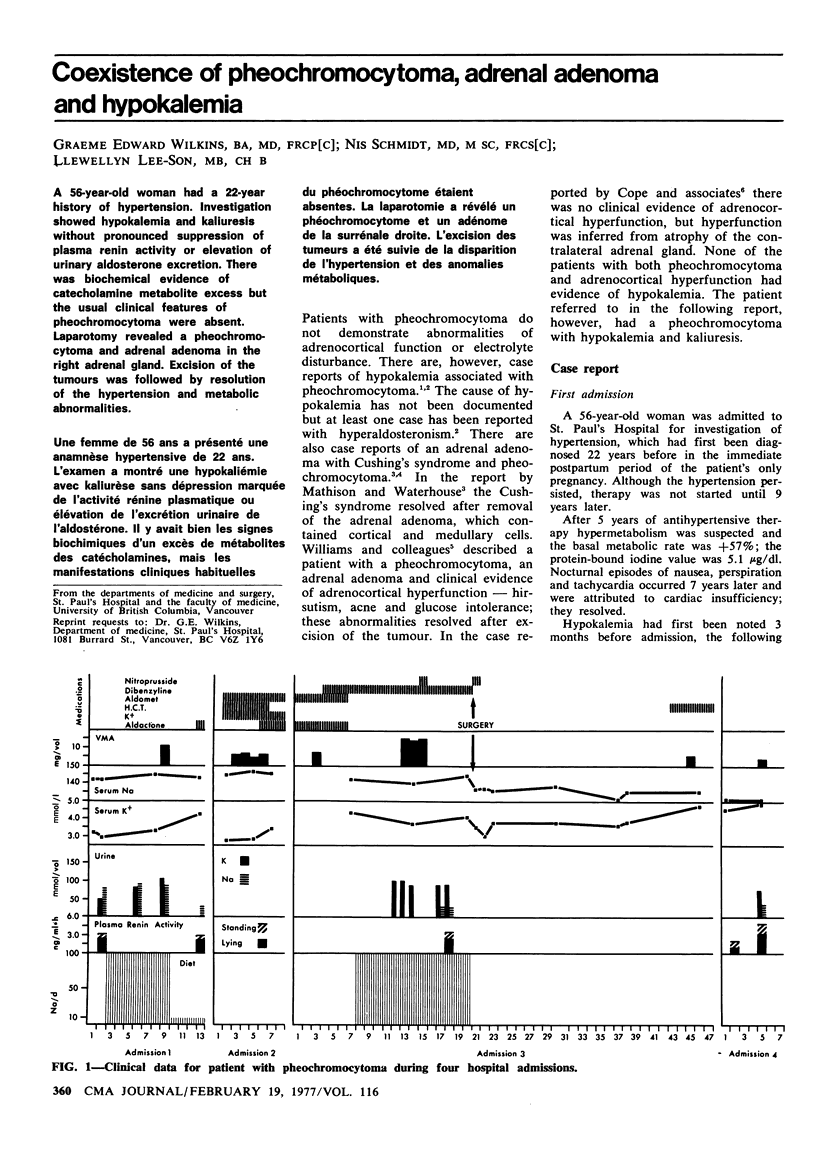
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- COPE O., LABBE J. P., RAKER J. W., BLAND E. F. Pheochromocytoma and adrenal cortical adenoma; report of a case with both tumors and discussion of their relation. J Clin Endocrinol Metab. 1952 Jul;12(7):875–880. doi: 10.1210/jcem-12-7-875. [DOI] [PubMed] [Google Scholar]
- Cain J. P., Tuck M. L., Williams G. H., Dluhy R. G., Rosenoff S. H. The regulation of aldosterone secretion in primary aldosteronism. Am J Med. 1972 Nov;53(5):627–637. doi: 10.1016/0002-9343(72)90158-1. [DOI] [PubMed] [Google Scholar]
- Granger P., Genest J. Autopsy study of adrenals in unselected normotensive and hypertensive patients. Can Med Assoc J. 1970 Jul 4;103(1):34–36. [PMC free article] [PubMed] [Google Scholar]
- Massara F., Tripodina A., Rotunno M. Propranolol block of epinephrine-induced hypokaliaemia in man. Eur J Pharmacol. 1970;10(3):404–407. doi: 10.1016/0014-2999(70)90214-1. [DOI] [PubMed] [Google Scholar]
- Mathison D. A., Waterhouse C. A. Cushing's syndrome with hypertensive crisis and mixed adrenal cortical adenoma-pheochromocytoma (corticomedullary adenoma). Am J Med. 1969 Oct;47(4):635–641. doi: 10.1016/0002-9343(69)90193-4. [DOI] [PubMed] [Google Scholar]
- Meloni C. R., Tucci J., Canary J. J., Kyle L. H. Cushing's syndrome due to bilateral adrenocortical hyperplasia caused by a benign adrenal medullary tumor. J Clin Endocrinol Metab. 1966 Nov;26(11):1192–1200. doi: 10.1210/jcem-26-11-1192. [DOI] [PubMed] [Google Scholar]
- NICKEL J. F., SMYTHE C. M., PAPPER E. M., BRADLEY S. E. A study of the mode of action of the adrenal medullary hormones on sodium, potassium and water excretion in man. J Clin Invest. 1954 Dec;33(12):1687–1699. doi: 10.1172/JCI103049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pheochromocytoma: current concepts of diagnosis and treatment. Combined clinical staff conference at the National Institutes of Health. Ann Intern Med. 1966 Dec;65(6):1302–1326. [PubMed] [Google Scholar]
- Reid I. A., Schrier R. W., Earley L. E. An effect of extrarenal beta adrenergic stimulation on the release of renin. J Clin Invest. 1972 Jul;51(7):1861–1869. doi: 10.1172/JCI106988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WILLIAMS G. A., CROCKETT C. L., BUTLER W. W., 3rd, CRISPELL K. R. The coexistence of pheochromocytoma and adrenocortical hyperplasia. J Clin Endocrinol Metab. 1960 Apr;20:622–631. doi: 10.1210/jcem-20-4-622. [DOI] [PubMed] [Google Scholar]
- Wilson R. J., Craig G. M., Mills I. H. Metabolic studies in a patient with a phaeochromocytoma associated with hypokalaemia and hyperaldosteronism. J Endocrinol. 1973 Jan;56(1):69–78. doi: 10.1677/joe.0.0560069. [DOI] [PubMed] [Google Scholar]