

Abstract
In a patient with a solitary pheochromocytoma severe hypoglycemia developed following excision of the tumour. The possible causative mechanism was thought to be a reactive relative increase in insulin production secondary to increased endogenous production of glucose, induced by the large amounts of epinephrine produced by the tumour. Alternatively, epinephrine withdrawal following removal of the tumour under phentolamine infusion may have induced increased insulin production and hence potentiated the development of hypoglycemia. Careful monitoring of the blood glucose concentration during and after the operation is recommended to obviate this potentially fatal complication.
Full text
PDF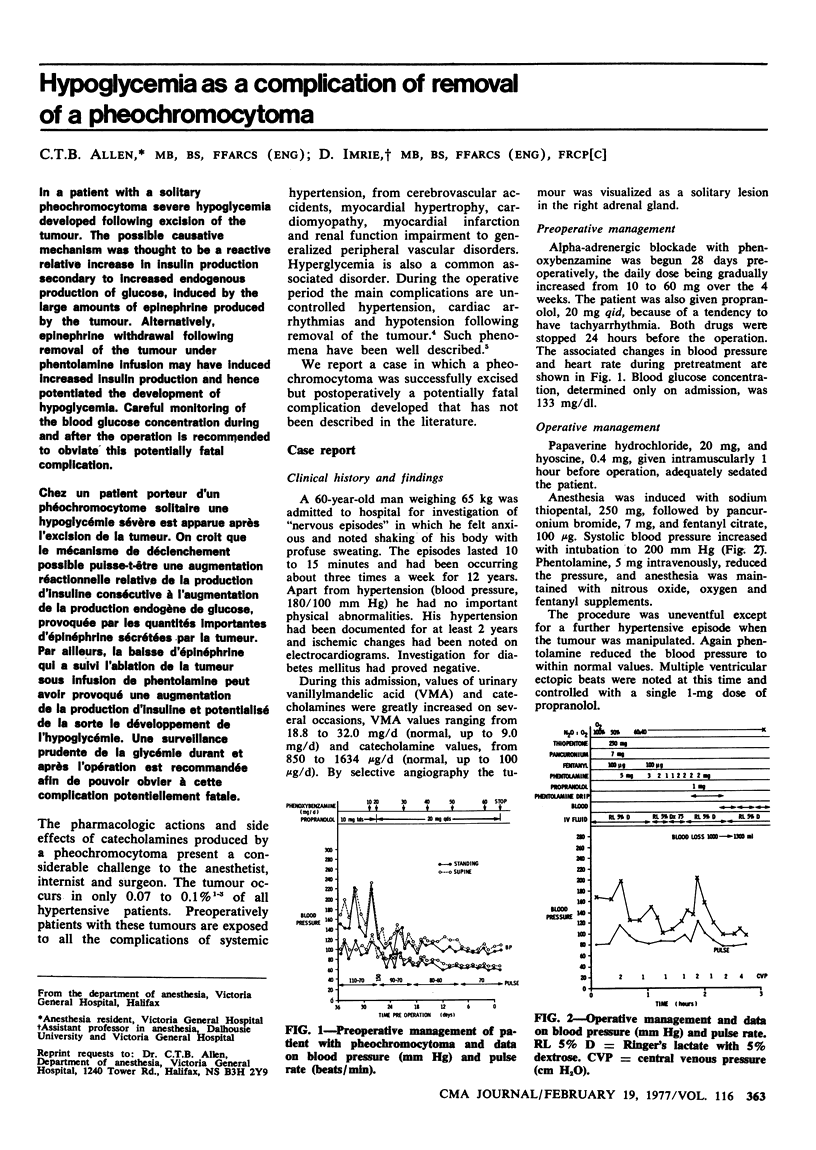
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Allison S. P., Prowse K., Chamberlain M. J. Failure of insulin response to glucose load during operation and after myocardial infarction. Lancet. 1967 Mar 4;1(7488):478–481. doi: 10.1016/s0140-6736(67)91097-5. [DOI] [PubMed] [Google Scholar]
- Cerasi E., Effendic S., Luft R. Role of adrenergic receptors in glucose-induced insulin secretion in man. Lancet. 1969 Aug 9;2(7615):301–302. doi: 10.1016/s0140-6736(69)90059-2. [DOI] [PubMed] [Google Scholar]
- Cooper C. E., Nelson D. H. ACTH LEVELS IN PLASMA IN PREOPERATIVE AND SURGICALLY STRESSED PATIENTS. J Clin Invest. 1962 Aug;41(8):1599–1605. doi: 10.1172/JCI104618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- FOLGER G. M., Jr, ROBERTS W. C., MEHRIZI A., SHAH K. D., GLANCY D. L., CARPENTER C. C., ESTERLY J. R. CYANOTIC MALFORMATIONS OF THE HEART WITH PHEOCHROMOCYTOMA. A REPORT OF FIVE CASES. Circulation. 1964 May;29:750–757. doi: 10.1161/01.cir.29.5.750. [DOI] [PubMed] [Google Scholar]
- GOLDENBERG I. S., HAYES M. A., GREENE N. M. Endocrine responses during operative procedures. Ann Surg. 1959 Aug;150(2):196–201. doi: 10.1097/00000658-195908000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- KVALE W. F., MANGER W. M., PRIESTLEY J. T., ROTH G. M. Pheochromocytoma. Circulation. 1956 Oct;14(4 Pt 1):622–630. doi: 10.1161/01.cir.14.4.622. [DOI] [PubMed] [Google Scholar]
- Lindseth R. E. Postoperative glucose metabolism in diabetic and nondiabetic patients. The response of glucose, insulin, growth hormone, corticosteroids, epinephrine, and unesterified fatty acids to extremity surgery. Arch Surg. 1972 Nov;105(5):741–745. doi: 10.1001/archsurg.1972.04180110064016. [DOI] [PubMed] [Google Scholar]
- Moffitt E. A., Schnelle N., Rodriguez R., Lee R. A., Judd E. S. Effects of intravenously administered solutions on electrolytes and energy substrates during surgery. Can Anaesth Soc J. 1974 May;21(3):285–293. doi: 10.1007/BF03005733. [DOI] [PubMed] [Google Scholar]
- Porte D., Jr, Graber A. L., Kuzuya T., Williams R. H. The effect of epinephrine on immunoreactive insulin levels in man. J Clin Invest. 1966 Feb;45(2):228–236. doi: 10.1172/JCI105335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Remine W. H., Chong G. C., Van Heerden J. A., Sheps S. G., Harrison E. G., Jr Current management of pheochromocytoma. Ann Surg. 1974 May;179(5):740–748. doi: 10.1097/00000658-197405000-00029. [DOI] [PMC free article] [PubMed] [Google Scholar]