

Abstract
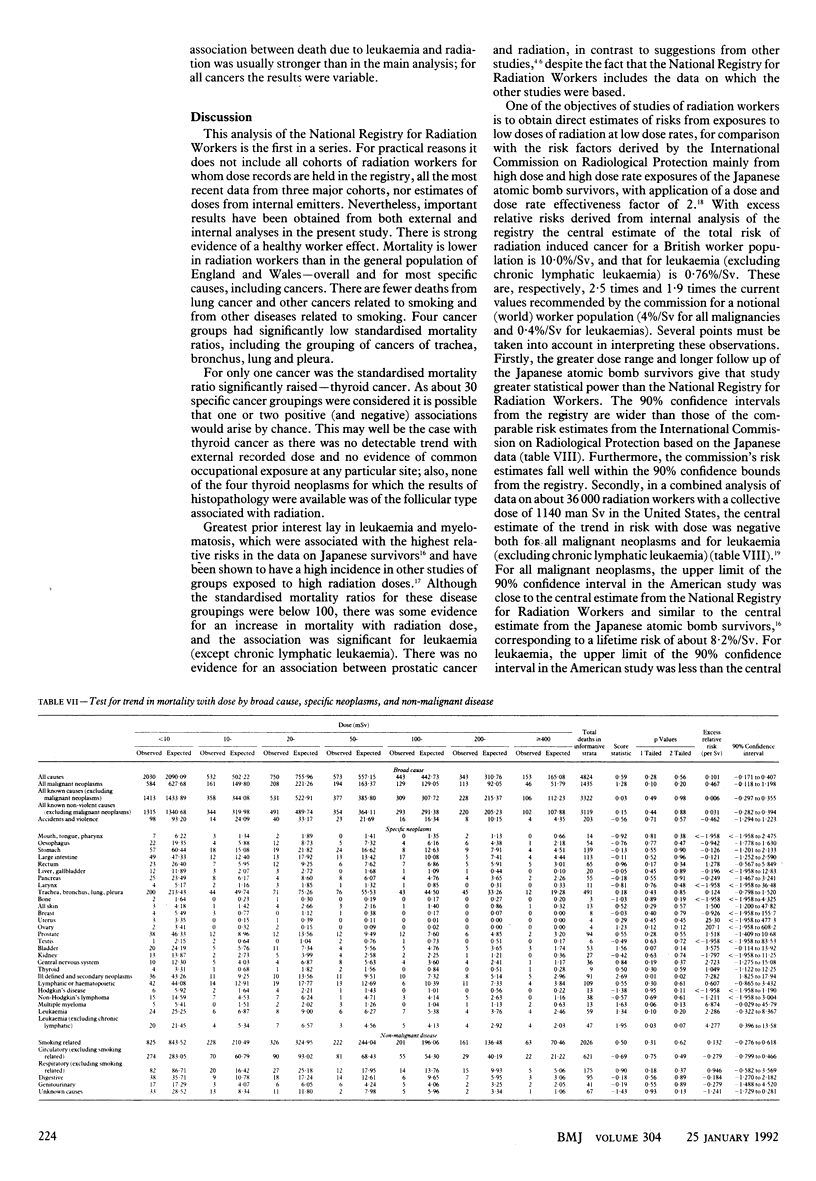
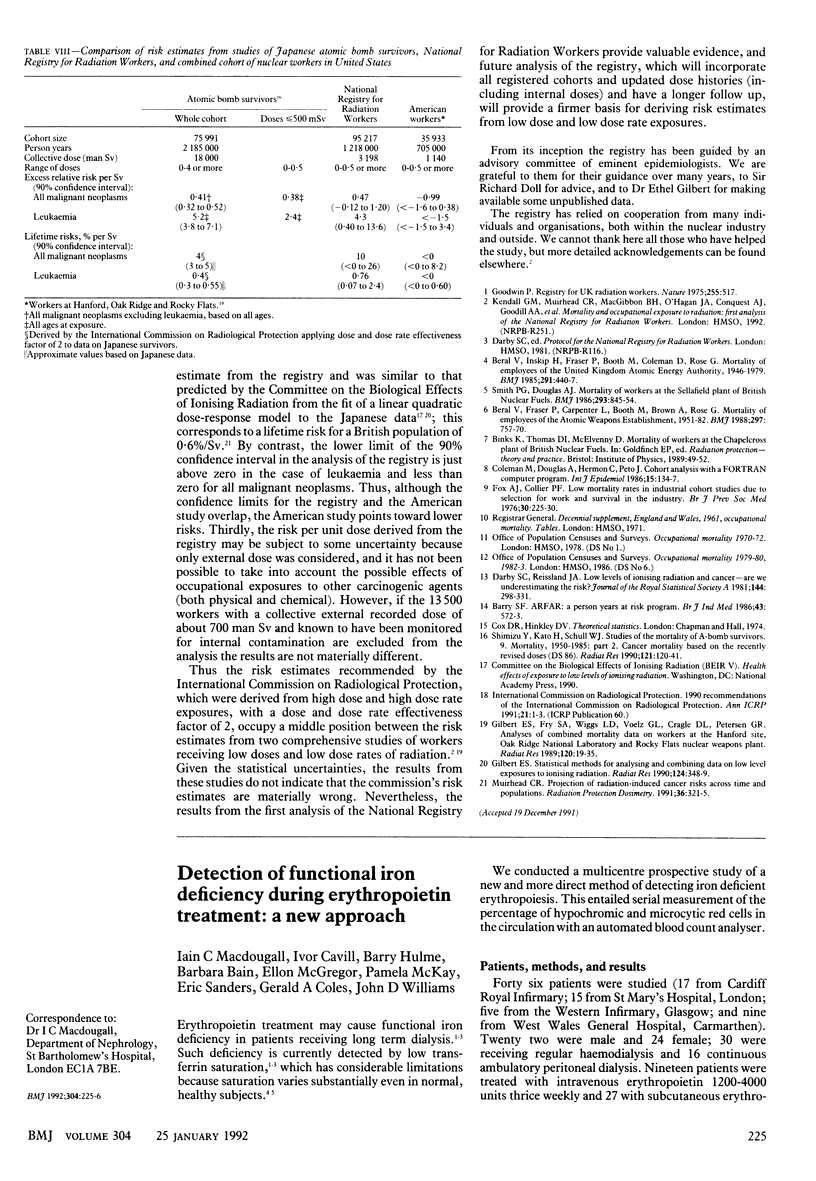
OBJECTIVE--To study cause specific mortality of radiation workers with particular reference to associations between fatal neoplasms and level of exposure to radiation. DESIGN--Cohort study. SETTING--United Kingdom. SUBJECTS--95,217 radiation workers at major sites of the nuclear industry. MAIN OUTCOME MEASURE--Cause of death. RESULTS--Most standardised mortality ratios were below 100: 83 unlagged, 85 with a 10 year lag for all causes; 84 unlagged, 86 lagged for all cancers; and 80 for all known other causes, indicating a "healthy worker effect." The deficit of lung cancer (75 unlagged, 76 lagged) was significant at the 0.1% level. Standardised mortality ratios were significantly raised (214 unlagged, 303 lagged) for thyroid cancer, but there was no evidence for any trend with external recorded radiation dose. Dose of external radiation and mortality from all cancers were weakly correlated (p = 0.10), and multiple myeloma was more strongly correlated (p = 0.06); for leukaemia, excluding chronic lymphatic, the trend was significant (p = 0.03; all tests one tailed). The central estimates of lifetime risk derived from these data were 10.0% per Sv (90% confidence interval less than 0 to 24%) for all cancers and 0.76% per Sv (0.07 to 2.4%) for leukaemia (excluding chronic lymphatic leukaemia). These are, respectively, 2.5 times and 1.9 times the risk estimates recommended by the International Commission on Radiological Protection, but 90% confidence intervals are large and the commission's risk factors fall well within the range. The positive trend with dose for all cancers, from which the risk estimate was derived, was not significant. The positive association between leukaemia (except chronic lymphatic leukaemia) was significant and robust in subsidiary analyses. This study showed no association between radiation exposure and prostatic cancer. CONCLUSION--There is evidence for an association between radiation exposure and mortality from cancer, in particular leukaemia (excluding chronic lymphatic leukaemia) and multiple myeloma, although mortality from these diseases in the study population overall was below that in the general population. The central estimates of risk from this study lie above the most recent estimates of the International Commission on Radiological Protection for leukaemia (excluding chronic lymphatic leukaemia) and for all malignancies. However, the commission's risk estimates are well within the 90% confidence intervals from this study. Analysis of combined cohorts of radiation workers in the United States indicated lower risk estimates than the commission recommends, and when the American data are combined with our analysis the overall risks are close to those estimated by the commission. This first analysis of the National Registry for Radiation Workers does not provide sufficient evidence to justify a revision in risk estimates for radiological protection purposes.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Barry S. F. ARFAR: a person years at risk program. Br J Ind Med. 1986 Aug;43(8):572–573. doi: 10.1136/oem.43.8.572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beral V., Fraser P., Carpenter L., Booth M., Brown A., Rose G. Mortality of employees of the Atomic Weapons Establishment, 1951-82. BMJ. 1988 Sep 24;297(6651):757–770. doi: 10.1136/bmj.297.6651.757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beral V., Inskip H., Fraser P., Booth M., Coleman D., Rose G. Mortality of employees of the United Kingdom Atomic Energy Authority, 1946-1979. Br Med J (Clin Res Ed) 1985 Aug 17;291(6493):440–447. doi: 10.1136/bmj.291.6493.440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coleman M., Douglas A., Hermon C., Peto J. Cohort study analysis with a FORTRAN computer program. Int J Epidemiol. 1986 Mar;15(1):134–137. doi: 10.1093/ije/15.1.134. [DOI] [PubMed] [Google Scholar]
- Fox A. J., Collier P. F. Low mortality rates in industrial cohort studies due to selection for work and survival in the industry. Br J Prev Soc Med. 1976 Dec;30(4):225–230. doi: 10.1136/jech.30.4.225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilbert E. S., Fry S. A., Wiggs L. D., Voelz G. L., Cragle D. L., Petersen G. R. Analyses of combined mortality data on workers at the Hanford Site, Oak Ridge National Laboratory, and Rocky Flats Nuclear Weapons Plant. Radiat Res. 1989 Oct;120(1):19–35. [PubMed] [Google Scholar]
- Shimizu Y., Kato H., Schull W. J. Studies of the mortality of A-bomb survivors. 9. Mortality, 1950-1985: Part 2. Cancer mortality based on the recently revised doses (DS86). Radiat Res. 1990 Feb;121(2):120–141. [PubMed] [Google Scholar]
- Smith P. G., Douglas A. J. Mortality of workers at the Sellafield plant of British Nuclear Fuels. Br Med J (Clin Res Ed) 1986 Oct 4;293(6551):845–854. doi: 10.1136/bmj.293.6551.845. [DOI] [PMC free article] [PubMed] [Google Scholar]