

Abstract
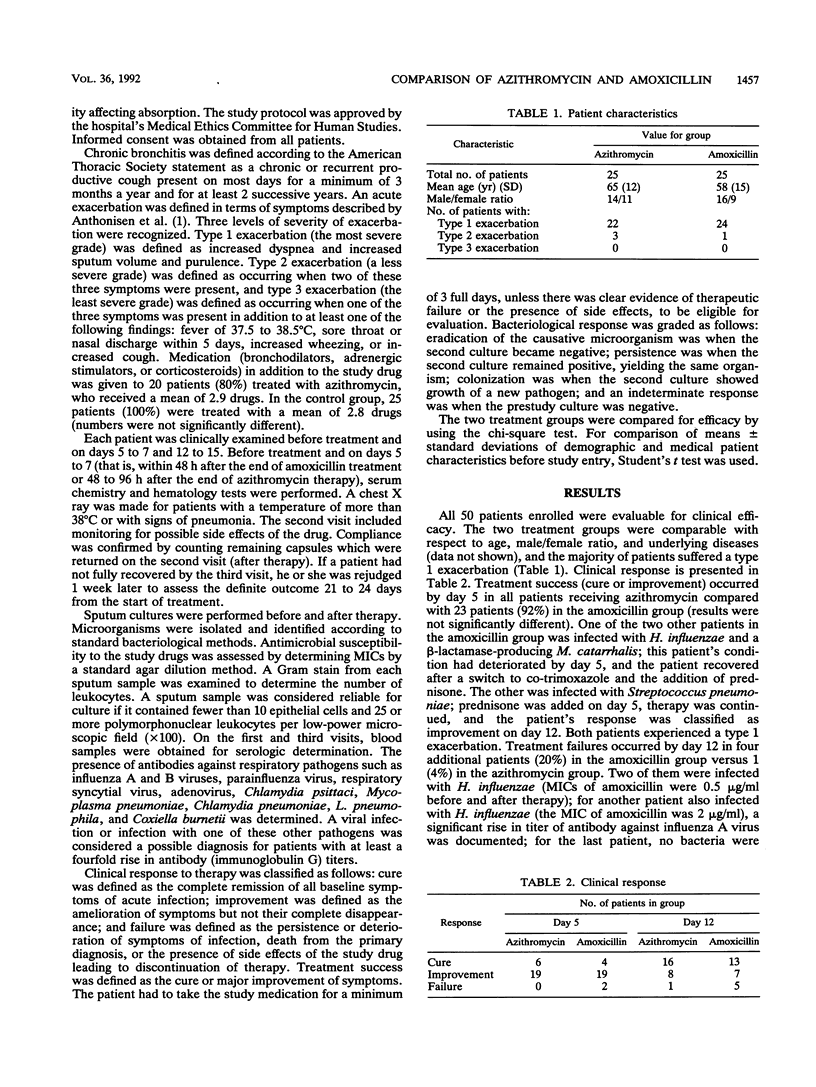
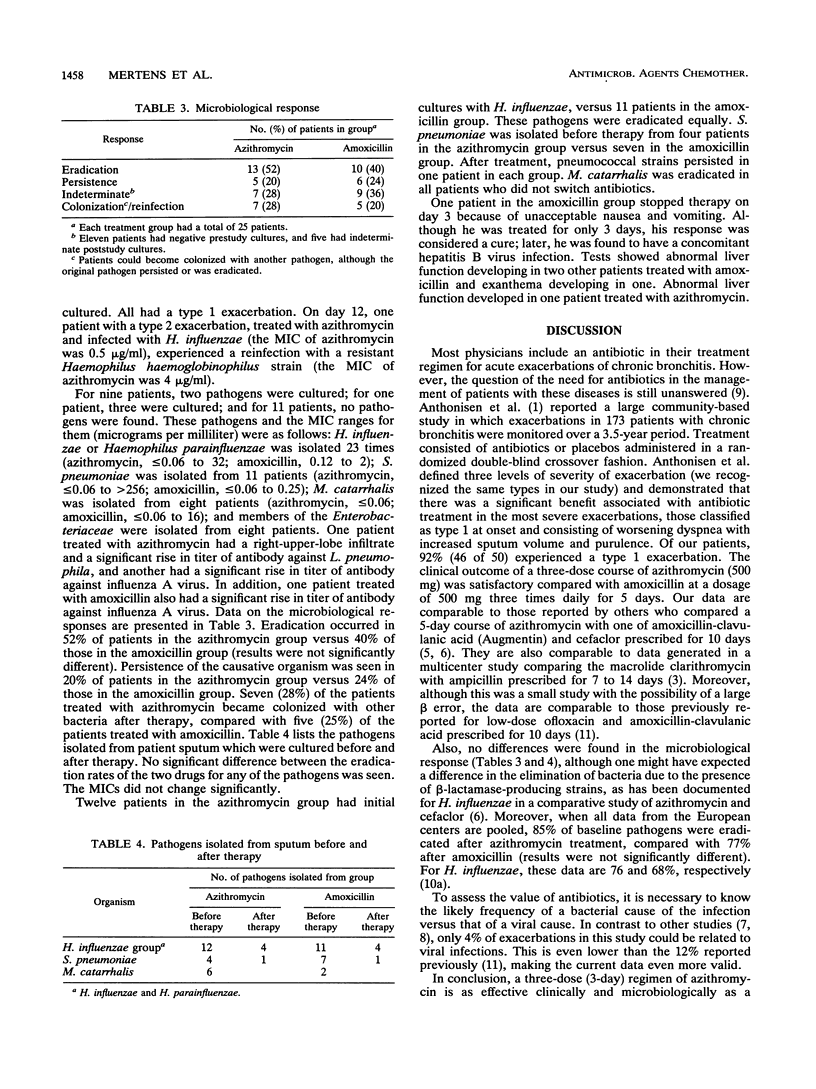
The efficacies and safeties of a three-dose regimen of azithromycin (500 mg once daily for 3 days) and a 15-dose regimen of amoxicillin (500 mg three times daily for 5 days) were compared in a double-blind manner in patients with an acute exacerbation of chronic bronchitis. A total of 92% of patients suffered a type 1 exacerbation. Treatment success, defined as cure or major improvement, was achieved in all patients in the azithromycin group by day 5, compared with 23 (92%) of 25 patients in the amoxicillin group. On day 12, these data were 24 of 25 (96%) in the azithromycin group and 20 of 25 (80%) in the amoxicillin group (results were not significantly different). Several pathogens were isolated (MIC ranges [micrograms per milliliter] in parentheses): Haemophilus influenzae or Haemophilus parainfluenzae was isolated 23 times (azithromycin, less than or equal to 0.06 to 32; amoxicillin, 0.12 to 2); Streptococcus pneumoniae was isolated from 11 patients (azithromcyin, less than or equal to 0.06 greater than 256; amoxicillin, less than or equal to 0.06 to 0.25); Moraxella (Branhamella) catarrhalis was isolated from eight patients (azithromycin, less than or equal to 0.06; amoxicillin, less than or equal to 0.06 to 16); and other members of the family Enterobacteriaceae were isolated from eight patients. One patient treated with azithromycin had Legionella pneumophila pneumonia, and another in that group had a significant rise in titer of antibody against influenza A virus. One patient treated with amoxicillin also had a significant rise in titer of antibody against influenza A virus. Microbiological response rates were comparable. One patient who received azithromycin developed abnormal liver function. Two patients treated with amoxicillin developed abnormal liver functions, one developed exanthema, and one treatment was stopped because of nausea. It is concluded that a three-dose (3-day) regimen of azithromycin is as effective clinically and microbiologically as a 15-dose (5-day) regimen of amoxicillin in the treatment of acute exacerbations of chronic bronchitis.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anthonisen N. R., Manfreda J., Warren C. P., Hershfield E. S., Harding G. K., Nelson N. A. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987 Feb;106(2):196–204. doi: 10.7326/0003-4819-106-2-196. [DOI] [PubMed] [Google Scholar]
- Azoulay-Dupuis E., Vallée E., Bedos J. P., Muffat-Joly M., Pocidalo J. J. Prophylactic and therapeutic activities of azithromycin in a mouse model of pneumococcal pneumonia. Antimicrob Agents Chemother. 1991 Jun;35(6):1024–1028. doi: 10.1128/aac.35.6.1024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bachand R. T., Jr Comparative study of clarithromycin and ampicillin in the treatment of patients with acute bacterial exacerbations of chronic bronchitis. J Antimicrob Chemother. 1991 Feb;27 (Suppl A):91–100. doi: 10.1093/jac/27.suppl_a.91. [DOI] [PubMed] [Google Scholar]
- Baldwin D. R., Wise R., Andrews J. M., Ashby J. P., Honeybourne D. Azithromycin concentrations at the sites of pulmonary infection. Eur Respir J. 1990 Sep;3(8):886–890. [PubMed] [Google Scholar]
- Balmes P., Clerc G., Dupont B., Labram C., Pariente R., Poirier R. Comparative study of azithromycin and amoxicillin/clavulanic acid in the treatment of lower respiratory tract infections. Eur J Clin Microbiol Infect Dis. 1991 May;10(5):437–439. doi: 10.1007/BF01968024. [DOI] [PubMed] [Google Scholar]
- Dark D. Multicenter evaluation of azithromycin and cefaclor in acute lower respiratory tract infections. Am J Med. 1991 Sep 12;91(3A):31S–35S. doi: 10.1016/0002-9343(91)90399-i. [DOI] [PubMed] [Google Scholar]
- Gump D. W., Phillips C. A., Forsyth B. R., McIntosh K., Lamborn K. R., Stouch W. H. Role of infection in chronic bronchitis. Am Rev Respir Dis. 1976 Apr;113(4):465–474. doi: 10.1164/arrd.1976.113.4.465. [DOI] [PubMed] [Google Scholar]
- Lamy M. E., Pouthier-Simon F., Debacker-Willame E. Respiratory viral infections in hospital patients with chronic bronchitis. Observations during periods of exacerbation and quiescence. Chest. 1973 Mar;63(3):336–341. doi: 10.1378/chest.63.3.336. [DOI] [PubMed] [Google Scholar]
- Neu H. C., Chin N. X., Saha G., Labthavikul P. Comparative in vitro activity of the new oral macrolide azithromycin. Eur J Clin Microbiol Infect Dis. 1988 Aug;7(4):541–544. doi: 10.1007/BF01962611. [DOI] [PubMed] [Google Scholar]
- Rademaker C. M., Sips A. P., Beumer H. M., Hoepelman I. M., Overbeek B. P., Möllers M. J., Rozenberg-Arska M., Verhoef J. A double-blind comparison of low-dose ofloxacin and amoxycillin/clavulanic acid in acute exacerbations of chronic bronchitis. J Antimicrob Chemother. 1990 Nov;26 (Suppl 500):75–81. doi: 10.1093/jac/26.suppl_d.75. [DOI] [PubMed] [Google Scholar]
- Retsema J., Girard A., Schelkly W., Manousos M., Anderson M., Bright G., Borovoy R., Brennan L., Mason R. Spectrum and mode of action of azithromycin (CP-62,993), a new 15-membered-ring macrolide with improved potency against gram-negative organisms. Antimicrob Agents Chemother. 1987 Dec;31(12):1939–1947. doi: 10.1128/aac.31.12.1939. [DOI] [PMC free article] [PubMed] [Google Scholar]