

Abstract
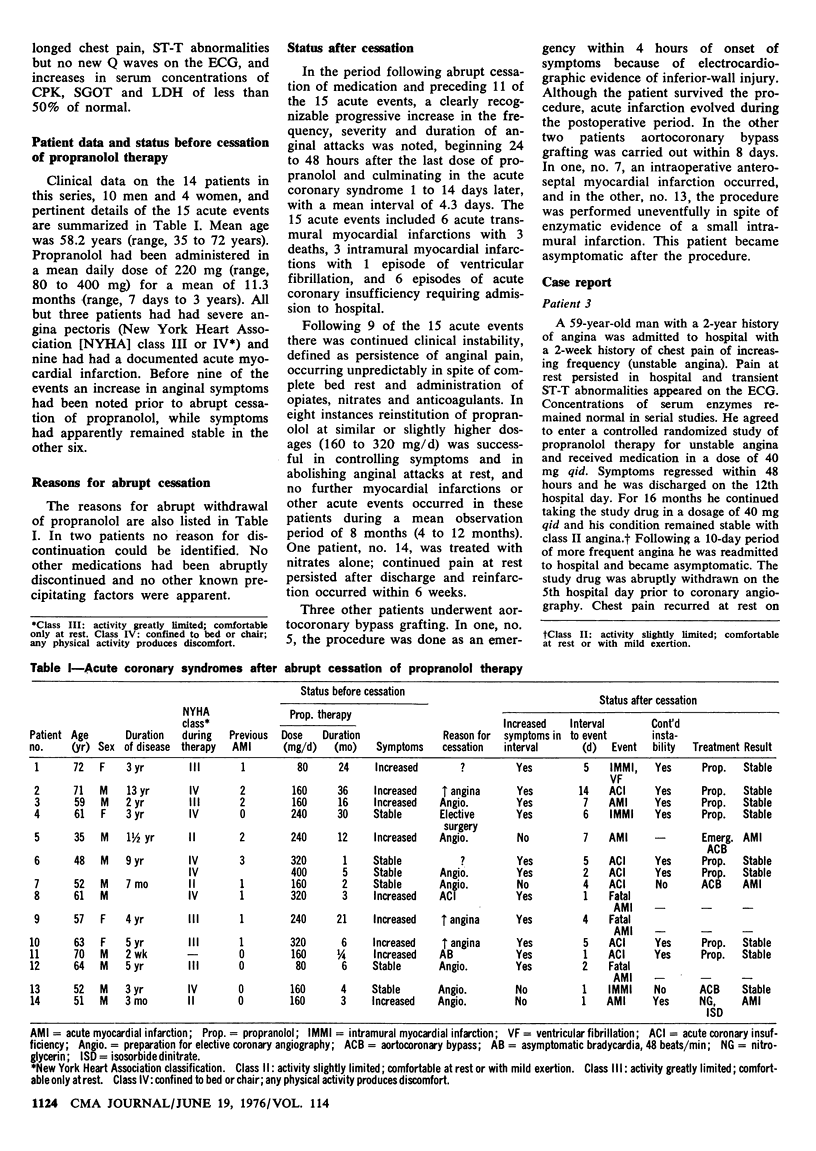
Abrupt cessation of oral propranolol therapy was followed by 15 acute coronary events in 14 patients with severe angina who had been receiving propranolol in daily doses of 80 to 400 mg for periods of 7 days to 6 years. Propranolol had been stopped 1 to 14 days before each acute event because of angiographic study (seven patients), increasing symptoms (three), acute coronary insufficiency (one), asymptomatic bradycardia (one), elective surgery (one) and unknown reasons (two). Before abrupt cessation of propranolol treatment anginal symptoms had been stable in six instances but had increased in the other nine. Cessation was followed by rapid progression of symptoms prior to 11 of the 15 acute events. There were six acute transmural myocardial infarctions with three deaths, three intramural myocardial infarctions, one with ventricular fibrillation, and six episodes of acute coronary insufficiency, Unstable angina followed nine of the events and responded to propranolol therapy (160 to 320 mg/d) in eight instances. Three other patients underwent aortocoronary bypass surgery; perioperative acute myocardial infarction occurred in two. These data suggest that in a minority of patients abrupt cessation of propranolol may be hazardous, particularly in severe or unstable disease. Cessation or propranolol therapy in such patients should be gradual and closely observed. Recurrent symptoms respond to reinstitution of propranolol therapy.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Diaz R. G., Somberg J., Freeman E., Levitt B. Myocardial infarction after propranolol withdrawal. Am Heart J. 1974 Aug;88(2):257–258. doi: 10.1016/0002-8703(74)90019-2. [DOI] [PubMed] [Google Scholar]
- Fischl S. J., Herman M. V., Gorlin R. The intermediate coronary syndrome: clinical, angiographic and therapeutic aspects. N Engl J Med. 1973 Jun 7;288(23):1193–1198. doi: 10.1056/NEJM197306072882301. [DOI] [PubMed] [Google Scholar]
- Gianelly R. E., Goldman R. H., Treister B., Harrison D. C. Propranolol in patients with angina pectoris. Ann Intern Med. 1967 Dec;67(6):1216–1225. doi: 10.7326/0003-4819-67-6-1216. [DOI] [PubMed] [Google Scholar]
- Mizgala H. F., Khan A. S., Davies R. O. Propranolol in the prophylactic treatment of angina pectoris. Can Med Assoc J. 1969 Apr 26;100(16):756–764. [PMC free article] [PubMed] [Google Scholar]
- Slome R. Withdrawal of propranolol and myocardial infarction. Lancet. 1973 Jan 20;1(7795):156–156. doi: 10.1016/s0140-6736(73)90235-3. [DOI] [PubMed] [Google Scholar]
- Viljoen J. F., Estafanous F. G., Kellner G. A. Propranolol and cardiac surgery. J Thorac Cardiovasc Surg. 1972 Nov;64(5):826–830. [PubMed] [Google Scholar]