

Abstract
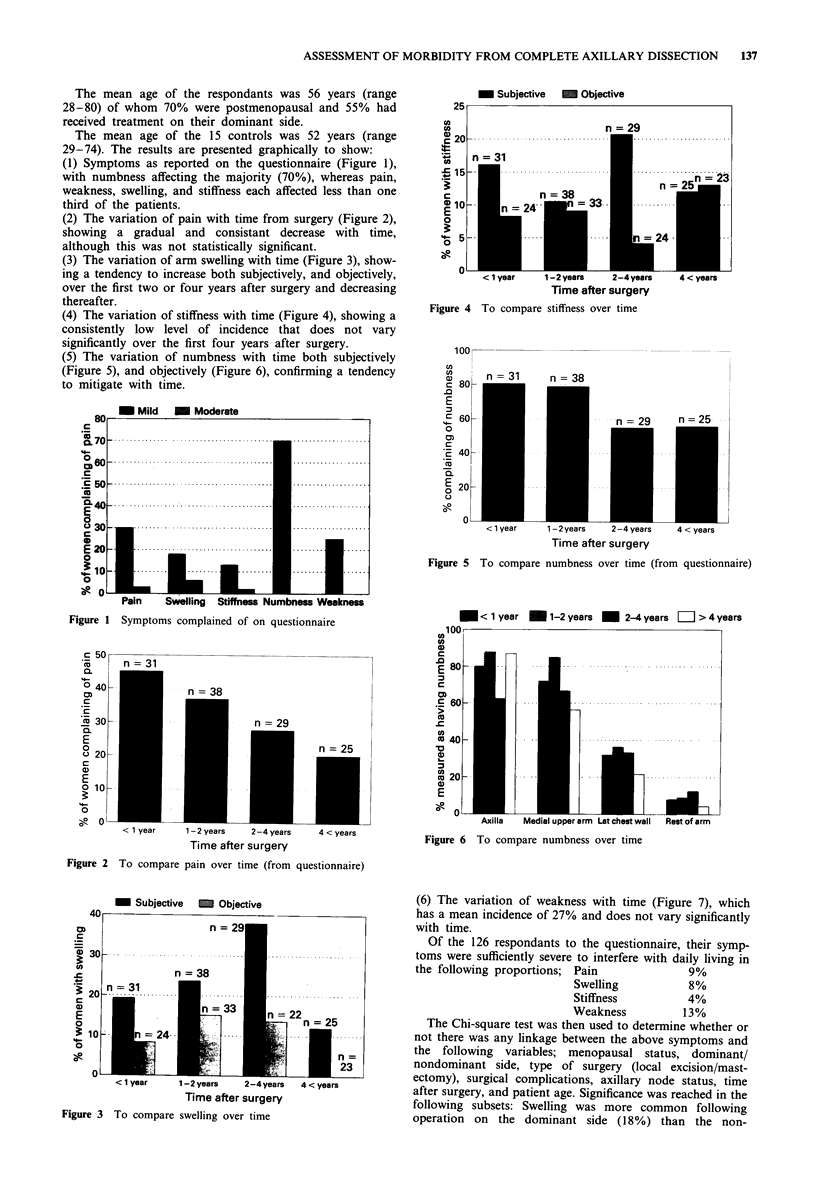
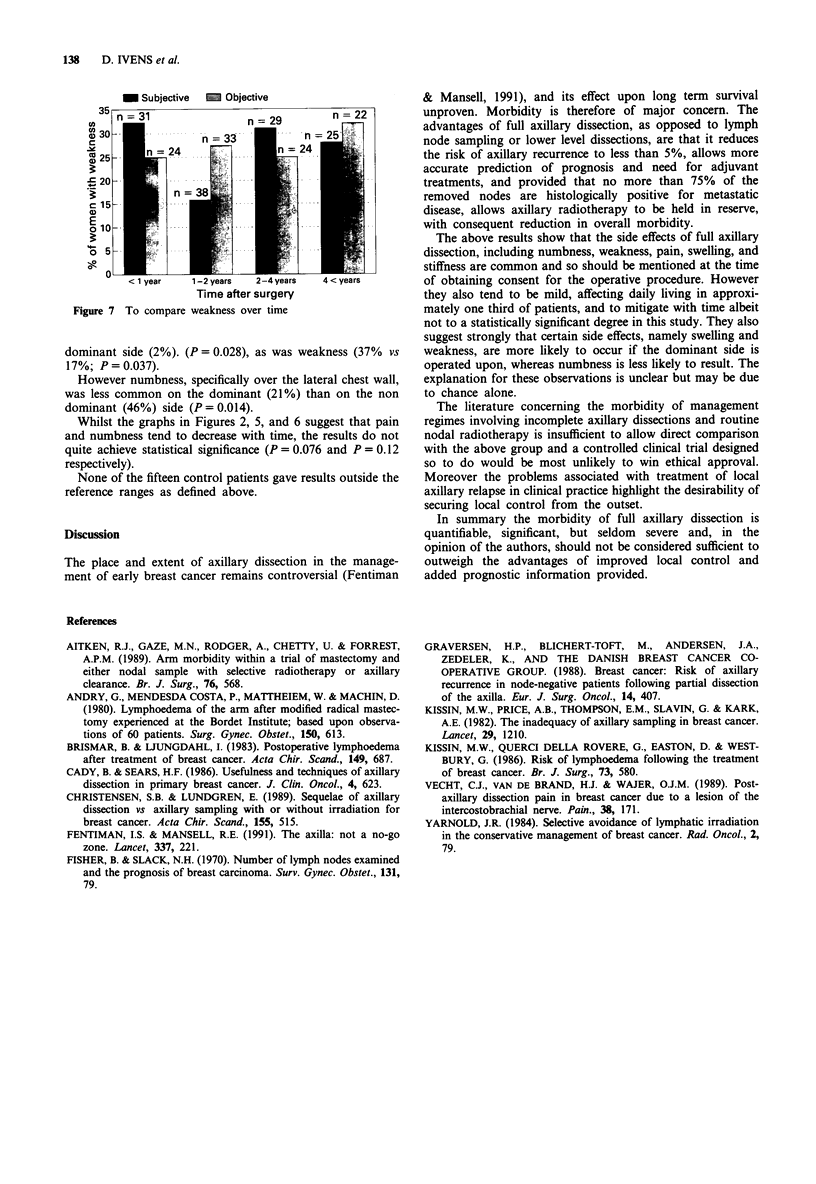
The importance of axillary dissection as part of the primary surgical procedure in the treatment of operable cases of carcinoma of the breast is established. The morbidity of this procedure, however, is less well documented. A study of 126 women who had had full axillary dissection as part of their initial surgical treatment was undertaken to assess their degree of morbidity in terms of numbness, pain, weakness, swelling, and stiffness. Seventy per cent of cases complained of numbness, 33% of pain, 25% of weakness, 24% of limb swelling, and 15% of stiffness. Objective measurements confirmed decreased sensation in 81%, weakness in 27%, swelling in 10%, and stiffness in 10%. In no case were these symptoms described as severe, though they did have an effect upon the daily lives of 39%. The side effects of full axillary dissection are common and all women should be warned of them prior to surgery; however they are usually mild and therefore should not preclude this procedure as a part of definitive surgical treatment.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aitken R. J., Gaze M. N., Rodger A., Chetty U., Forrest A. P. Arm morbidity within a trial of mastectomy and either nodal sample with selective radiotherapy or axillary clearance. Br J Surg. 1989 Jun;76(6):568–571. doi: 10.1002/bjs.1800760613. [DOI] [PubMed] [Google Scholar]
- Borup Christensen S., Lundgren E. Sequelae of axillary dissection vs. axillary sampling with or without irradiation for breast cancer. A randomized trial. Acta Chir Scand. 1989 Oct;155(10):515–519. [PubMed] [Google Scholar]
- Brismar B., Ljungdahl I. Postoperative lymphoedema after treatment of breast cancer. Acta Chir Scand. 1983;149(7):687–689. [PubMed] [Google Scholar]
- Cady B., Sears H. F. Usefulness and technique of axillary dissection in primary breast cancer. J Clin Oncol. 1986 May;4(5):623–624. doi: 10.1200/JCO.1986.4.5.623. [DOI] [PubMed] [Google Scholar]
- Fentiman I. S., Mansel R. E. The axilla: not a no-go zone. Lancet. 1991 Jan 26;337(8735):221–223. doi: 10.1016/0140-6736(91)92172-x. [DOI] [PubMed] [Google Scholar]
- Fisher B., Slack N. H. Number of lymph nodes examined and the prognosis of breast carcinoma. Surg Gynecol Obstet. 1970 Jul;131(1):79–88. [PubMed] [Google Scholar]
- Graversen H. P., Blichert-Toft M., Andersen J. A., Zedeler K. Breast cancer: risk of axillary recurrence in node-negative patients following partial dissection of the axilla. Eur J Surg Oncol. 1988 Oct;14(5):407–412. [PubMed] [Google Scholar]
- Kissin M. W., Querci della Rovere G., Easton D., Westbury G. Risk of lymphoedema following the treatment of breast cancer. Br J Surg. 1986 Jul;73(7):580–584. doi: 10.1002/bjs.1800730723. [DOI] [PubMed] [Google Scholar]
- Kissin M. W., Thompson E. M., Price A. B., Slavin G., Kark A. E. The inadequacy of axillary sampling in breast cancer. Lancet. 1982 May 29;1(8283):1210–1212. doi: 10.1016/s0140-6736(82)92337-6. [DOI] [PubMed] [Google Scholar]
- Vecht C. J., Van de Brand H. J., Wajer O. J. Post-axillary dissection pain in breast cancer due to a lesion of the intercostobrachial nerve. Pain. 1989 Aug;38(2):171–176. doi: 10.1016/0304-3959(89)90235-2. [DOI] [PubMed] [Google Scholar]
- Yarnold J. R. Selective avoidance of lymphatic irradiation in the conservative management of breast cancer. Radiother Oncol. 1984 Aug;2(2):79–92. doi: 10.1016/s0167-8140(84)80043-2. [DOI] [PubMed] [Google Scholar]