

Abstract
Context: Ankle sprains are a common basketball injury. Therefore, examination of risk factors for injury in female professional basketball players is worthwhile.
Objective: To examine rates of ankle sprains, associated time missed from participation, and risk factors for injury during 2 consecutive seasons.
Design: Prospective cohort study.
Setting: Eighteen professional basketball facilities.
Patients or Other Participants: We observed 204 players from 18 female professional basketball teams for 2 consecutive seasons during a 2-year period.
Main Outcome Measure(s): Using questionnaires, we recorded the incidence of ankle sprains, participation time missed, and mechanisms of injury in games and practice sessions. Potential risk factors, such as age, body mass, height, training experience, and history of ankle sprain, were examined using multivariate logistic regression.
Results: Fifty of the 204 participants sustained ankle injuries; injuries included 32 ankle sprains, which translated to an ankle sprain rate of 1.12 per 1000 hours of exposure to injury. The 32 players missed 224.4 training and game sessions and an average of 7.01 sessions per injury. Most injuries occurred in the key area of the basketball court and were the result of contact. Injury rates during games were higher than injury rates during practice sessions. Centers, followed by guards and forwards, had the highest rate of injury. Players who did not wear an external ankle support had an odds ratio of 2.481 for sustaining an ankle sprain.
Conclusions: Female professional basketball athletes who did not wear an external ankle support, who played in the key area, or who functioned as centers had a higher risk for ankle sprain than did other players.
Keywords: risk factors, team sports, injury epidemiology, injury prevention
Key Points
Female professional basketball players who wear external ankle supports can significantly reduce the risk of sustaining an ankle sprain.
A history of ankle sprain was a risk factor for reinjury.
Most ankle sprains occurred with contact, in centers, and inside the key area of the basketball court.
Age, height, training experience, body mass, and history of previous ankle sprain were not significant predictors of injury.
Basketball is a fast and aggressive game, and its participants have one of the highest overall injury rates among participants in noncollision sports. 1–3 For this reason, interest in the type and mechanism of basketball-related injuries has grown.
Ankle sprain is one of the most common injuries in basketball players 4–6 and is caused by frequent jumps, landings, cutting maneuvers, and contact with other players, all of which are inherent parts of the sport. Investigators 6–8 have reported that basketball players have a high rate of recurrence of ankle sprain. To our knowledge, many authors 7, 9 have examined ankle sprains in amateur basketball players. However, few investigators have examined professional players, and their studies mainly have focused on American basketball players. 4, 10, 11 In theory, professional players demonstrate higher fitness and technique levels than do amateurs. High fitness levels combined with more aggressive play may result in more contacts between players and more movements and, therefore, in a higher risk of injury. Because ankle sprain is a common basketball injury, examination of the risk factors for injury in professional players is worthwhile.
Examination of risk factors for injury in female athletes is particularly important because women may have higher rates of injury than men. 2, 4, 9, 10, 12 For example, Hosea et al 5 reported that, compared with male athletes, female collegiate athletes were at 25% increased risk of sustaining a grade I ankle sprain. Therefore, identification of risk factors for ankle sprains in this category of basketball players is important.
Researchers have identified numerous factors that may cause injury, including the age of the player, 4, 7, 13 injury conditions (during practice or game), 7, 13, 14 factors in body size, 7, 9 history of previous injury, 8, 9, 15 mechanism of injury (contact or noncontact), 7, 13, 14, 16 use of external ankle support, 15, 17–19 and player position. 4, 7, 13, 15, 17 These issues, either individually or in different combinations, may contribute to the occurrence of injury.
Research findings on the effects of age on injury rates are conflicting 4, 7, 20; some authors report increased injury rates in older players, 4, 20 and other authors report no effects of age. 7 Exposure to injury over time in older players is greater than in younger athletes, 20 so injury rates in older players are likely to be greater as well. However, other factors may influence the role of age as a risk factor for injury. Of these factors, training experience of the player is particularly important because it provides information about the years of previous exposure of each player. 4 In theory, players with more training experience have a longer history of exposure to injury, so they may demonstrate a higher rate of injury. However, players with more experience demonstrate better technical skills and lower injury rates. In addition, some researchers have shown that body size and anthropometric characteristics also may affect the risk of injury, 21 but other researchers have asserted the opposite. 4, 22
Two factors that may affect the risk of ankle sprain are use of external ankle support 19, 20 and history of ankle sprain. 6, 11, 19, 21 Investigators have shown that external ankle support may prevent injury 6, 11, 19 and that a previous strain or sprain on the same side of the ankle is a strong predictor for reinjury. 6–11, 19, 21 Athletes who have a history of ankle sprain and who use a brace or tape appear to have a lower incidence of ankle sprain, 6–11, 19, 21 which indicates that the interaction between these 2 factors affects the occurrence of injury.
Beynnon et al 21 concluded that investigators are divided about whether age, height, and mass are risk factors for ankle sprain. They recommended that more research be done in this area. To our knowledge, research focusing on ankle sprains in female players and the relation to these factors is not clear. Furthermore, investigators have shown that the relative risk of ankle injury doubles with an increased level of competition, from scholastic to collegiate play. 13, 17 If the risk does double, then female professional basketball players would have an even higher risk of injury than athletes participating at lower levels of competition.
The purpose of our study was to examine the rates of ankle sprains, associated time lost from participation, and the risk factors for injury during 2 consecutive seasons of the Greece Women's National Basketball Association. In particular, we examined the characteristics and mechanisms of ankle sprains and analyzed the individual and combined roles of age, height, body mass, type of external ankle support, and history of previous injury as risk factors for ankle sprain.
METHODS
Eighteen of the 28 professional basketball clubs in the Greece Women's National Basketball Association volunteered to participate in our study. Player injuries were monitored prospectively for 2 years (from August 2003 to August 2005). Using a player injury audit questionnaire designed for this study, physiotherapists or medical doctors or both recorded injuries. Before the study, full-time medical staff from each club attended a course regarding the project methods and received specific guidelines regarding completion of the questionnaire. Before each season, athletes were required to give written consent. Of the 216 athletes who were eligible for enrollment in the study, 204 (94.4%) provided written consent. We recorded basic medical information and anthropometric data on these athletes (age = 24.8 ± 4.63 years, height = 1.75 ± 0.09 m, mass = 65.5 ± 5.75 kg, training experience = 7.6 ± 4.02 years, body mass index = 20.3 ± 5.17). We also recorded the playing position for the athletes: there were 51 (25.0%) point guards, 26 (12.7%) guards, 61 (29.9%) small forwards, 30 (14.7%) power forwards, and 36 (17.7%) centers. The study was approved by the local university ethics committee.
We defined a reportable injury as an injury that occurred during training or competition and that prevented the injured player from participating in practice sessions or games. Injuries unrelated to basketball and absences resulting from illness were not included. We divided injuries, as noted on a weekly exposure sheet, into 2 categories based on severity: injuries resulting in loss of participation for fewer than 7 sessions and injuries resulting in loss of participation for 7 or more sessions. Reinjury was defined as an injury of the same nature and location in the same player during the same season.
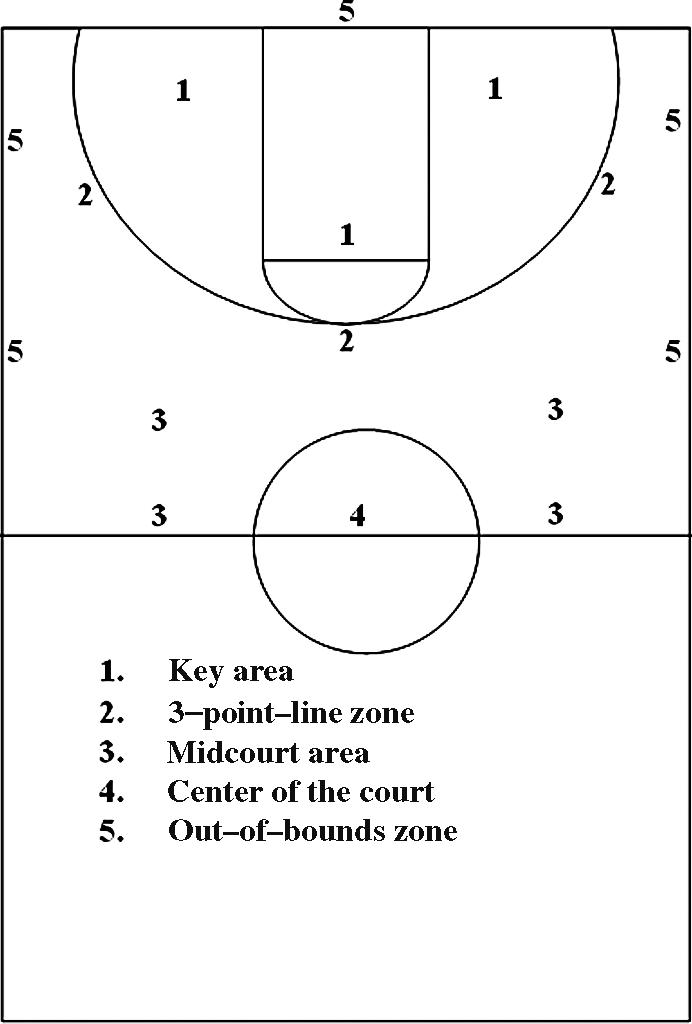
During the season, individual participation, hours of exposure to injury, and any injury data were registered daily using a standardized questionnaire. Injury audit questionnaires were used to record information about each basketball player for each exposure in practices and games. A physical therapist used a weekly sheet in tabular form to document the participation status; hours of exposure to injury; and various conditions of injury occurrence including injury area (region in which injury occurred), session type (game or practice), player position (guard, forward, or center), date of injury (month), injury mechanism (contact or noncontact), previous ankle sprain, and placement of external joint support (taping or joint support). The therapist also recorded the court zone in which the injury took place ( Figure 1). The level of participation of each player during each game and practice session was recorded and expressed in hours of exposure to injury.
Figure 1. The 5 areas of the basketball court: 1, the key (defined by the free throw line); 2, the 3-point–line zone; 3, the midcourt area; 4, the center of the court; and 5, the out-of-bounds zone.
At the beginning of each season, we taught the medical staff of each basketball team how to identify the type and region of injury. With this knowledge, the staff made these identifications during practice sessions and games. Qualified medical doctors made all diagnostic decisions. Sample diagnosis forms were checked among teams for consistency. 23 Methods of diagnosis were monitored throughout the study and in most cases (71.7%) included radiographic and physical examination. The remaining injuries were diagnosed using magnetic resonance imaging.
The full-time physiotherapists and physicians, in collaboration with an assistant we provided, registered injury data each day. The assistant also recorded the daily practice and participation time. In addition, we discussed and cross-checked the records each week. In most cases, the same person was collecting data for each team for the entire study period.
Individual exposure to injury also was registered for each session by describing each exposure as full time, partial, or none. Time lost from participation because of an ankle sprain was calculated on the basis of missed games or practice sessions. In addition, explanatory codes identified the reasons for time lost and were designated as sprain injured, sick, or absent for reasons other than injury or illness. We examined the weekly data forms for completeness and entered the information into Access 2003 (Microsoft Inc, Redmond, WA).
Data Analysis
The rate of injury was assessed as the number of injuries per 1000 hours of exposure. We further analyzed the risk factors associated with age, height, body mass, training experience, injury severity, injury area, practice session versus game, timing of ankle sprains, mechanism of injury, previous injury, and use of external ankle support.
For each variable, we calculated descriptive statistics. We used χ 2 tests to investigate the significant difference between the recorded values and their expected distribution at P < .05. More specifically, we used the χ 2 test to examine differences in frequency of injuries in various ankle regions, with contact and without contact, with various contact or noncontact mechanisms of injury, in games and practice sessions, at different court zones, and at different playing positions.
We considered data on age, training status, body mass, height, history of previous ankle sprain, and use of external ankle support in a backward, stepwise, multivariate logistic regression analysis to evaluate potential predictor variables. For each variable, the odds ratio was estimated as the odds of exposure to injury among injured athletes compared with the odds of exposure among the controls. The odds ratio for those players who had a history of ankle sprain and who did not wear external supports was calculated. The level of significance was set at P < .05.
RESULTS
During the 2 years of the study, we documented 50 ankle injuries, which included 32 ankle sprains. These 32 injuries resulted in 224.4 missed participation sessions. The proportion of injured athletes was 15.7%. The average time lost per injury was 7.01 sessions.
We observed 936 games and 5040 practice sessions during the 2-year study. On average, each team practiced 4.35 ± 0.24 sessions and played 0.81 ± 0.16 games per week. We observed all players for an average of 35.69 hours of exposure to injury, including 30.34 hours during practice and 5.35 hours during games. On average, each player practiced 2.32 ± 0.54 hours per week and played 0.41 ± 0.11 hours per week in games. This average does not include the number of sessions missed as a result of injury or for other reasons.
Region of Injury
The 32 ankle sprains accounted for 64% of the total ankle injuries (n = 50) sustained during the 2 seasons ( P = .007) ( Table 1). Ankle sprain was the most common injury that caused athletes to lose fewer than 7 sessions ( P = .007). Achilles tendinitis was the most common injury that caused athletes to lose 7 or more sessions ( Table 1).
Table 1. Injury Rate and Severity by Ankle Region.

Type and Mechanisms of Ankle Sprain
Table 2 shows the mechanism of each sprain as either contact or noncontact. Most sprains occurred through contact ( P = .001). More contact injuries than noncontact injuries led to fewer than 7 sessions missed. Player contact accounted for 78.3% of contact ankle sprains and 56.3% of all ankle sprains ( P = .001). In addition, 77.7% of noncontact ankle sprains occurred during landing or with twisting and turning.
Table 2. Ankle Injury Rate by Mechanism and Severity.

Games Versus Practices
Table 3 shows a breakdown of injury frequency and injury rate for game and practice sessions. The absolute number of injuries in practice sessions was significantly more than the number during games (χ 2 1 = 14.12, P = .028). However, the rate of injury was much higher in games than in practice sessions (χ 2 1 = 17.11, P = .013).
Table 3. Ankle Injury Frequency and Severity by Exposure Type (Games and Practices).

Ankle Sprains and Mechanisms by Court Area and Player Position
Table 4 provides an analysis of the frequency and rate of injury by court zone. The largest number of injuries occurred in the key area, which accounted for 56.3% ( P = .007) of all ankle sprains, at a rate of 0.45 injuries per 1000 hours of exposure to injury. Among the player positions examined, small forwards had the lowest rate of injury, and centers had the highest rate of injury ( Table 5; χ 2 2,4 = 9.99, P = .043).
Table 4. Ankle Injury Rate and Severity by Court Zone.

Table 5. Frequency and Rate of Common Ankle Injuries by Player Position.

Injury Occurrence During a Season
We observed that 53.2% (n = 17) of ankle sprains occurred during the first 2 months of the season. The injury rate was much higher (χ 2 7 = 18.0, P = .012) in these months than in the remaining months of the season ( P = .012) ( Table 6).
Table 6. Month During Which Ankle Sprain Occurred.

Injuries With or Without External Support
We found that 54.90% (n = 112) of the participants wear ankle joint supports ( Figure 2). We also found that 9.82% (n = 11) of players who wore joint supports sustained ankle sprains, and 22.9% (n = 21) of the players who did not wear any type of support were injured (χ 2 1 = 6.48, P = .001).
Figure 2. Number of participants who were injured and were not injured while wearing and not wearing external ankle support.

History of Injury
Of the participants, 67.6% (n = 138) had a previous ankle injury ( Figure 3). Of these players, 17.39% (n = 24) sustained a new injury. Of the 64 players without a history of previous injury, 12.5% (n = 8) sustained an ankle sprain (χ 2 1 = 1.41, P = .333) ( Figure 3).
Figure 3. Number of injured and noninjured participants with and without a history of ankle sprain.

History of Injury and Use of External Support
The results also showed that the odds ratio for those players who had a history of ankle sprain and who did not wear external ankle support was 4.013 (confidence interval = 0.891, 4.775).
Multivariate Logistic Regression
The multivariate logistic regression analysis showed that external support was a significant predictor of ankle sprain ( P = .0002), with an odds ratio of 2.481 ( Table 7). History of previous injury, age, body mass, height, and years of training experience were not significant predictors ( P > .05). Of these variables, we found it interesting that the odds ratio for sprain in players who experienced a previous sprain was high (1.675).
Table 7. Odds Ratios and Confidence Intervals Resulting From the Multivariate Logistic Regression Model.

DISCUSSION
Rates and Mechanisms of Injury
During a 2-year period, 204 professional female basketball players had 50 ankle injuries, resulting in 224.4 (practice and game) sessions missed ( Table 1), which corresponds with the findings of other investigators. 4, 7, 13, 16, 17
Ankle sprains were the most common injury that resulted in less than 7 missed sessions, and tendinitis was the most common injury that resulted in 7 or more missed sessions ( Table 1). No uniform consensus exists on how long injured ligaments take to reach normal tensile strength. 24 Pain resolves more quickly with a sprain, allowing a faster return to play. Tendinitis tends to be a chronic rather than an acute injury, resulting in longer symptomatic periods. In our study, players may have returned to full function without restoration of full tensile strength of the ligament. This difference in duration of symptoms could explain why players were absent longer from games or training when they had tendinitis than when they had an ankle sprain.
Most injuries occurred with contact ( Table 2), which corresponds with the findings in other studies. 7, 14 The rate of contact injuries was much higher than the rate of noncontact injuries, which clearly indicates the close contact among female players during games and practices. In our study, most contact injuries resulted from contact with another player ( Table 2), which is in agreement with the findings of Hickey et al. 14 Yde and Nielsen 25 found that contact with the ball itself, followed by contact with an opponent, was responsible for the largest number of contact injuries. However, their sample included athletes from 3 ball games, so direct comparison with our findings is difficult.
We observed noncontact ankle sprains during landing, twisting and turning, collision, and falling ( Table 2). Injuries sustained in these ways could be attributed to the fact that these movements are very frequent in basketball, 6 and they may induce high joint and musculoskeletal forces. 17, 18 McKay et al 17 observed that 45% of the ankle injuries in their study's participants occurred during landing on another player's foot or on the court surface.
The absolute number of injuries in practice was higher than that observed during games, but the rate of injury was much higher in games than in practices ( Table 3). Our results correspond with the results of Junge et al 22 and Meeuwisse et al, 13 who found that injuries occurred 3.7 times more often in games than during practices. However, Messina et al 16 found smaller differences in injury rates between games and practices in 1863 male and female high school basketball players. The higher rate of injury during games could be attributed to the increased player contact and aggression during games. 22
The largest number of injuries occurred within the key area of the basketball court ( Table 4). This result could be attributed to the amount of time athletes play in the key area, which results in more exposure time, and to the fact that game play inside the key area involves jumps, landings (from jump shots, layups, and rebounds), and player-to-player contact (in defense or offense). This result also can explain the higher injury rates in the centers ( Table 5), who spend most of their playing time in the key area, either in defense or offense. Meeuwisse et al 13 reported similar results for collegiate basketball players.
Risk Factors
Our results indicate that age is not a significant predictor of injury ( Table 7). Comparison among studies is difficult because of differences in the sports and age ranges of the subjects examined as well as differences in the method used to examine the effects of age. For example, Stevenson et al 26 found that athletes aged 26 to 30 years were at 55% increased risk of injury compared with athletes who were less than 26 years and more than 30 years of age. McKay et al 17 reported that, compared with older athletes (average age = 28 years), younger athletes (average age = 25.2 years) were at increased risk of sustaining ankle injury. Among 13 age groups, Starkey 4 reported that injury risk was higher for players aged less than 20 years, but it increased for players from 38 to 40 years of age. In our study, we treated age as a continuous variable and examined it using regression, but authors of other studies 7, 20 divided their samples into age categories. Furthermore, our sample had a wide age distribution, but the relatively small number of injuries may have made observing an association between age and injury difficult.
In our study, anthropometric variables, such as body mass and height, were also not significant predictors of injury. This finding could be related to homogeneity of our sample on anthropometric measures. It is in contrast to the findings of Emery et al 27 in soccer players. However, Beynnon et al 28 examined collegiate athletes and found that height and weight were not independent risk factors for ankle sprains. Sitler et al 18 reported similar findings for basketball players. McKay et al 17 did not find a significant difference in height or weight among elite and recreational basketball players who incurred ankle injuries and those who did not. Starkey 4 reported an increased risk of game injury for overweight players studied for 10 years. This finding may be a result of examining a larger and more heterogeneous sample size than the sample size that we examined in our study. For the specific sample that we examined, the results indicate that anthropometric variables were not significant predictors of ankle sprains in female professional basketball players.
Our results indicated the odds ratio for a player with a history of ankle sprain to sustain another injury was 1.675 ( Figure 3). This finding corresponds with findings in other studies of basketball players 6, 19 and has been attributed to various factors, including proprioception deficits; muscle strength impairments and imbalance; persistent ligamentous laxity; diminished muscle flexibility and joint movement; and the presence of localized scar tissue, which produces discomfort. 29 Disruption of a ligament compromises an important biomechanical stabilizer and creates partial deafferentation of the ankle. 18, 30 Investigators have shown that neuromuscular control of the ankle joint is reduced in athletes reporting instability after injury 18 and even in the immediate recovery period after an acute injury. 26 In contrast, authors of other studies 31, 32 have reported that athletes with a previous ankle injury do not demonstrate increased risk for a new injury. The disparity among studies may be related to the definition of injury, to different techniques of injury assessment, and to differences in the quality of rehabilitation treatment provided to the samples of players examined. Our results, however, indicate that female professional basketball players who sustained an ankle sprain were more likely to sustain a second injury. Arnason et al 33 commented that the increased risk of injury is partly due to early return to sport. Our experience during this 2-year project was that athletes and coaches often choose an early return to sport, accompanied by interruption of the rehabilitation program. We believe that completion of the rehabilitation program after ankle sprain is critical for avoiding recurrence of injury.
In our study, we found that most injuries occurred when players did not wear ankle supports ( Figure 2), which is in agreement with previously reported data. 6, 19, 25 The results from the logistic regression model indicated that female basketball players who did not wear external supports demonstrated an odds ratio of 2.481 for sustaining an ankle sprain. Researchers 5, 15, 25 also have reported increased incidence of noncontact injury when players do not wear external ankle supports. For example, Sitler et al 18 examined collegiate basketball athletes and reported a lower incidence of ankle sprains in athletes who had a history of ankle sprains and who wore a brace. McKay et al 17 also studied basketball players and reported that using ankle tape for support decreased the risk of reinjury in athletes with a history of ankle sprains. The protective mechanisms of wearing external support were attributed to enhancement of mechanical support 7 and restriction in range of motion. 19, 34 Investigators 7, 11, 15, 19, 21, 25 have shown that athletes who have a history of ankle sprain and who use a brace or tape experience a lower incidence of ankle sprains. The high odds ratio (4.013) displayed by the players who had a history of ankle sprains and who did not wear external supports further confirms the reported observations.
Direct comparison of the injury rate in our study with the rates found by other investigators is difficult because of various factors, such as a different definition of the rate of injury, competition level, and sex of the players. Most researchers have expressed injury rate as the number of injuries per 1000 athlete-exposures. 4, 6, 11, 13, 28 Assuming that 1 athlete-exposure equals 0.66 hours of exposure, 11 the injury rate in our study could be approximated to a value of 1.68 per 1000 athlete-exposures. For game conditions, the rate would be approximately 2.52 per 1000 athlete-exposures. This value is lower than the value reported for players of the Women's National Basketball Association (4.3 per 1000 athlete-exposures 11) and for players of the National Basketball Association (3.4 per 1000 athlete-exposures 4). In contrast, the rate is similar to 6 or higher than 13, 28 rates reported for high school and collegiate players. These differences can be attributed to several factors; the most important factor is differences in the level of competition examined. Research has indicated a higher injury rate in professional players than in collegiate basketball players. 35 Consequently, we suggest that, compared with high school and collegiate players, the professional players examined in our study played at a higher level of competition and had more game experience, 13, 28 so they demonstrated higher rates of injury. However, their level of play might not have been as intensive as that seen for American professional basketball players, 4, 11 so we observed lower rates of injury than did other investigators. 4, 11
Beynnon et al 21 indicated that the effect of sex on the rate of ankle injury is not as evident as this effect on the rate of knee injuries. Researchers have examined sex differences in the rates of ankle sprain in professional basketball players 11, 15, 22 and have found similar rates of ankle injury for men and women. Comparison of these studies with our study is difficult because of the effects of other factors, such as the level of skill, game experience, and intensity of play. For example, as stated, the injury rate observed in participants in our study is lower than the rate observed for both male and female American professional players. 4, 11 This finding excludes sex from being considered as a factor responsible for this difference. Further research is needed to examine the effect of sex on injury rates in female and male players matched for similar training characteristics.
Our longitudinal study was limited because although total sample size was relatively high, the number of recorded injuries limited our ability to draw conclusions regarding the role of risk factors in predicting injury. For the specific sport that we examined, sample size was determined, among other ways, based on the number of registered professional basketball players in a country, by the willingness of the subjects to participate, and by the drop-out rate of the final participants. In our study, we recorded approximately 64% of professional athletes playing in the same league, of whom 6.6% (n = 12) did not finish the study. Determination of the statistically appropriate sample size in identifying risk factors in our study would require examination of all teams playing in this league, which in practical terms is a difficult task.
Clinical Implications
We found that based on the variety of factors examined, external joint support and history of previous ankle sprain affect the risk of ankle sprain. Our results indicate that the occurrence of ankle sprain in female professional players could be reduced significantly if players wore external joint supports. The evidence regarding the type of ankle support to be used is not entirely conclusive, 19 but we believe that female basketball players, especially those players who already have sustained an ankle sprain, would benefit from wearing external supports.
CONCLUSIONS
We found that female professional basketball players had an ankle sprain rate of 1.12 per 1000 hours of exposure to injury. Players demonstrated a higher rate of contact injuries during games than in practices. Most injuries took place inside the key area, and centers had a much higher rate of injury than did players participating in other positions. Logistic regression also indicated that age, height, training experience, body mass, and history of previous ankle sprain were not significant predictors of injury. However, players who did not wear external supports had an odds ratio for sustaining an ankle sprain of 2.481. Injury prevention strategies in female basketball players should focus on the use of external ankle supports, especially during games. This strategy applies in particular to those athletes who play in the key area of the court, mostly centers, and to those athletes who have experienced an ankle sprain.
REFERENCES
- Whiteside PA. Men's and women's injuries in comparable sports. Physician Sportsmed. 1980;8(3):130–140. doi: 10.1080/00913847.1980.11948586. [DOI] [PubMed] [Google Scholar]
- DeHaven KE, Lintner DM. Athletic injuries: comparison by age, sport, and gender. Am J Sports Med. 1986;14:218–224. doi: 10.1177/036354658601400307. [DOI] [PubMed] [Google Scholar]
- Weesner CL, Albohm MJ, Ritter MA. A comparison of anterior and posterior cruciate ligament laxity between female and male basketball players. Physician Sportsmed. 1986;14(5):149–154. doi: 10.1080/00913847.1986.11709076. [DOI] [PubMed] [Google Scholar]
- Starkey C. Injuries and illnesses in the National Basketball Association: a 10-year perspective. J Athl Train. 2000;35:161–167. [PMC free article] [PubMed] [Google Scholar]
- Hosea TM, Carey CC, Harrer MF. The gender issue: epidemiology of ankle injuries in athletes who participate in basketball. Clin Orthop Relat Res. 2000;372:45–49. doi: 10.1097/00003086-200003000-00006. [DOI] [PubMed] [Google Scholar]
- McGuine TA, Greene JJ, Best T, Leverson G. Balance as a predictor of ankle injuries in high school basketball players. Clin J Sport Med. 2000;10:239–244. doi: 10.1097/00042752-200010000-00003. [DOI] [PubMed] [Google Scholar]
- Gomez E, DeLee JC, Farney WC. Incidence of injury in Texas girls' high school basketball. Am J Sports Med. 1996;24:684–687. doi: 10.1177/036354659602400521. [DOI] [PubMed] [Google Scholar]
- Payne KA, Berg K, Latin RW. Ankle injuries and ankle strength, flexibility, and proprioception in college basketball players. J Athl Train. 1997;32:221–225. [PMC free article] [PubMed] [Google Scholar]
- Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. Am J Sports Med. 1995;23:694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- Colliander E, Eriksson E, Herkel M, Skold P. Injuries in Swedish elite basketball. Orthopedics. 1986;9:225–227. doi: 10.3928/0147-7447-19860201-14. [DOI] [PubMed] [Google Scholar]
- Deitch JR, Starkey C, Walters SL, Moseley JB. Injury risk in professional basketball players: a comparison of Women's National Basketball Association and National Basketball Association athletes. Am J Sports Med. 2006;34:1077–1083. doi: 10.1177/0363546505285383. [DOI] [PubMed] [Google Scholar]
- Ireland ML, Wall C. Epidemiology and comparison of knee injuries in elite male and female United States basketball injuries. Med Sci Sports Exerc. 1990;22:S82. (suppl) [Google Scholar]
- Meeuwisse WH, Sellmer R, Hagel B. Rates and risks of injury during intercollegiate basketball. Am J Sports Med. 2003;31:379–385. doi: 10.1177/03635465030310030901. [DOI] [PubMed] [Google Scholar]
- Hickey GJ, Fricker PA, McDonald WA. Injuries of young elite female basketball players over a six-year period. Clin J Sport Med. 1997;7:252–256. doi: 10.1097/00042752-199710000-00002. [DOI] [PubMed] [Google Scholar]
- Zelisko JA, Noble HB, Porter M. A comparison of men's and women's professional basketball injuries. Am J Sports Med. 1982;10:297–299. doi: 10.1177/036354658201000507. [DOI] [PubMed] [Google Scholar]
- Messina DF, Farney WC, DeLee JC. The incidence of injury in Texas high school basketball: a prospective study among male and female athletes. Am J Sports Med. 1999;27:294–299. doi: 10.1177/03635465990270030401. [DOI] [PubMed] [Google Scholar]
- McKay GD, Goldie PA, Payne WR, Oakes BW. Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med. 2001;35:103–108. doi: 10.1136/bjsm.35.2.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sitler M, Ryan J, Wheeler B. The efficacy of a semirigid ankle stabilizer to reduce acute ankle injuries in basketball: a randomized clinical study at West Point. Am J Sports Med. 1994;22:454–461. doi: 10.1177/036354659402200404. et al. [DOI] [PubMed] [Google Scholar]
- Olmsted LC, Vela LI, Denegar CR, Hertel J. Prophylactic ankle taping and bracing: a numbers-needed-to-treat and cost-benefit analysis. J Athl Train. 2004;39:95–100. [PMC free article] [PubMed] [Google Scholar]
- Leanderson J, Wykman A, Eriksson E. Ankle sprain and postural sway in basketball players. Knee Surg Sports Traumatol Arthrosc. 1993;1:203–205. doi: 10.1007/BF01560207. [DOI] [PubMed] [Google Scholar]
- Beynnon BD, Murphy DF, Alosa DM. Predictive factors for lateral ankle sprains: a literature review. J Athl Train. 2002;37:376–380. [PMC free article] [PubMed] [Google Scholar]
- Junge A, Langevoort G, Pipe A. Injuries in team sport tournaments during the 2004 Olympic Games. Am J Sports Med. 2005;34:565–576. doi: 10.1177/0363546505281807. et al. [DOI] [PubMed] [Google Scholar]
- Heyworth J. Ottawa ankle rules for the injured ankle. Br J Sports Med. 2003;37:194. doi: 10.1136/bjsm.37.3.194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Callaghan MJ. Role of ankle taping and bracing in the athlete. Br J Sports Med. 1997;31:102–108. doi: 10.1136/bjsm.31.2.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yde J, Nielsen AB. Sports injuries in adolescents' ball games: soccer, handball and basketball. Br J Sports Med. 1990;24:51–54. doi: 10.1136/bjsm.24.1.51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevenson MR, Hamer P, Finch CF, Elliot B, Kresnow M. Sport, age, and sex specific incidence of sports injuries in Western Australia. Br J Sports Med. 2000;34:188–194. doi: 10.1136/bjsm.34.3.188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emery CA, Meeuwisse WH, Hartmann SE. Evaluation of risk factors for injury in adolescent soccer: implementation and validation of an injury surveillance system. Am J Sports Med. 2005;33:1882–1891. doi: 10.1177/0363546505279576. [DOI] [PubMed] [Google Scholar]
- Beynnon BD, Renstrom PA, Alosa DM, Baumhauer JR, Vacek PM. Ankle ligament injury risk factors: a prospective study of college athletes. J Orthop Res. 2001;19:213–220. doi: 10.1016/S0736-0266(00)90004-4. [DOI] [PubMed] [Google Scholar]
- Sitler MR, Horodyski M. Effectiveness of prophylactic ankle stabilisers for prevention of ankle injuries. Sports Med. 1995;20:53–57. doi: 10.2165/00007256-199520010-00005. [DOI] [PubMed] [Google Scholar]
- Konradsen L, Voigt M. Inversion injury biomechanics in functional ankle instability: a cadaver study of simulated gait. Scand J Med Sci Sports. 2002;12:329–336. doi: 10.1034/j.1600-0838.2002.00108.x. [DOI] [PubMed] [Google Scholar]
- Konradsen L, Olesen S, Hansen HM. Ankle sensorimotor control and eversion strength after acute ankle inversion injuries. Am J Sports Med. 1998;26:72–77. doi: 10.1177/03635465980260013001. [DOI] [PubMed] [Google Scholar]
- Tropp H, Odenrick P, Gillguist J. Stabilometry recordings in functional and mechanical instability of the ankle joint. Int J Sports Med. 1985;6:180–182. doi: 10.1055/s-2008-1025836. [DOI] [PubMed] [Google Scholar]
- Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R. Risk factors for injuries in football. Am J Sports Med. 2004;32:5S–16S. doi: 10.1177/0363546503258912. [DOI] [PubMed] [Google Scholar]
- Cordova ML, Ingersoll CD, Palmieri RM. Efficacy of prophylactic ankle support: an experimental perspective. J Athl Train. 2002;37:446–457. [PMC free article] [PubMed] [Google Scholar]
- Vicente R. National Collegiate Athletic Association. 1981–82–2004–05 NCAA Sports Sponsorship and Participation Rates Report . Available at: http://www.ncaa.org/library/research/participation_rates/1982-005/1982_2005_participation_rates.pdf. Accessed May 2, 2007 .