

Abstract
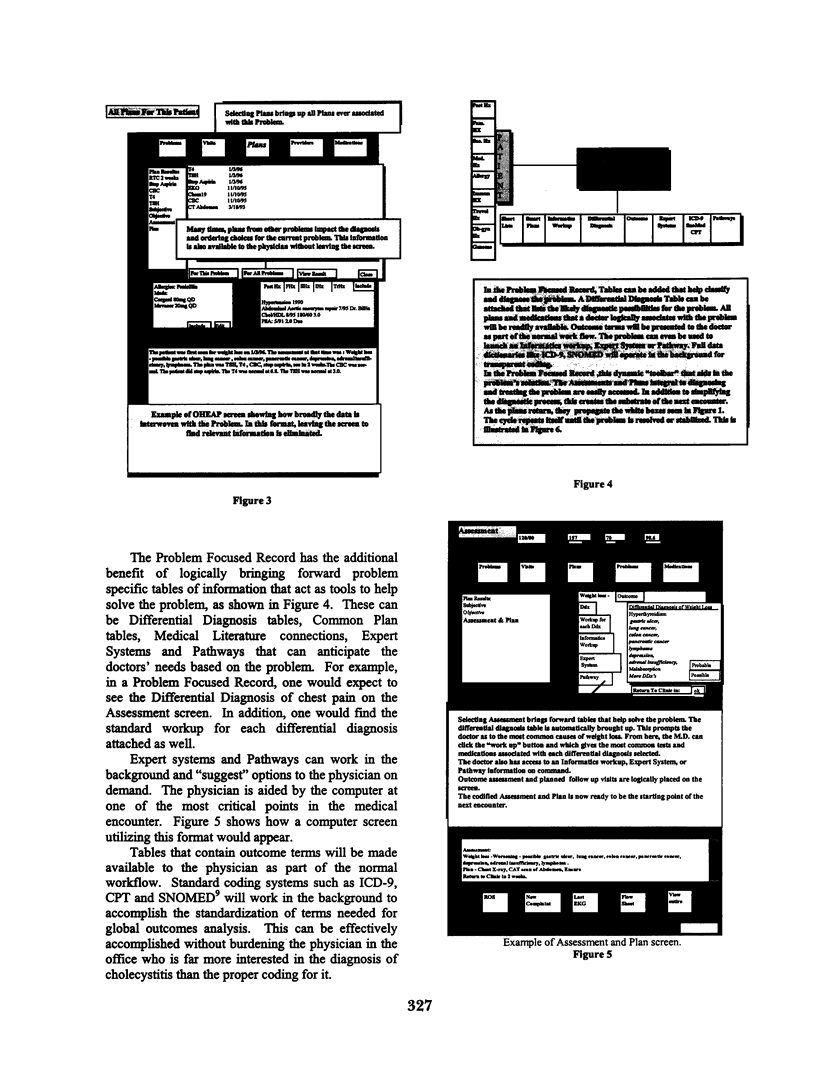
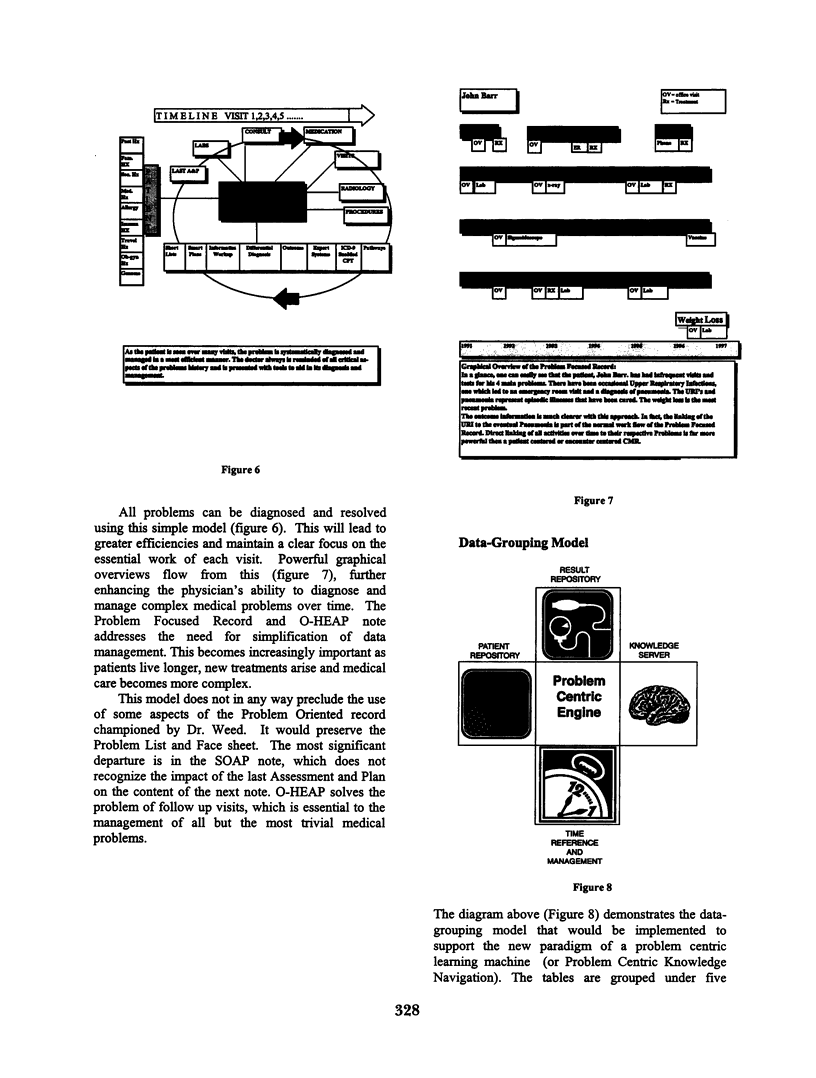
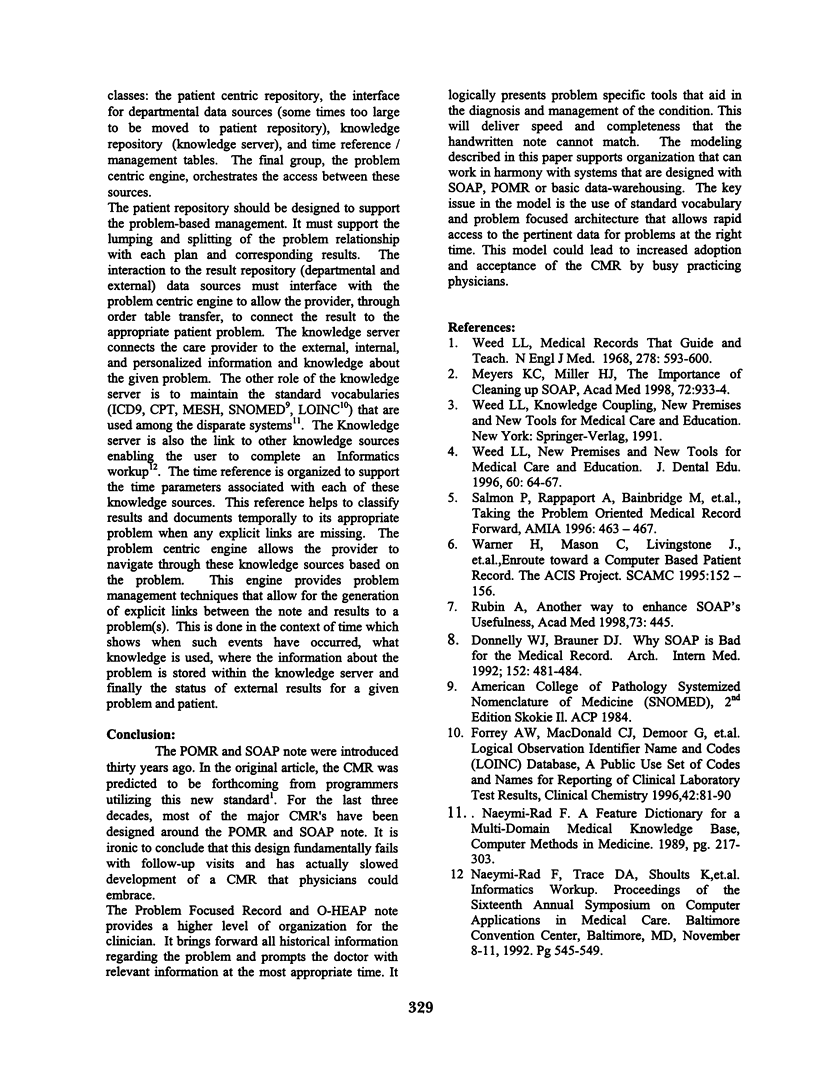
The current organization of most Computerized Medical Records (CMR) is based on the Problem Oriented Medical Record (POMR) and the SOAP (Subjective, Objective, Assessment and Plan) note. The organizational structure of the POMR and especially the SOAP note, does not allow for optimal use of computer capabilities in the follow up note. Since follow up visits are the most common office visit by far, this is a major flaw in the CMR. The authors propose a Problem Focused Medical Record and the OHEAP (Orientation, History, Exam, Assessment and Plan) note to resolve this problem. OHEAP starts with a powerful orientation structure that brings forward the timeline, last Assessment and Plan, and Plan Results for each problem along with the patient's historical tables as the starting point of every follow up visit. The Assessment and Plan portion brings problem specific differential diagnoses and their workups along with other relevant tables such as expert systems, treatments, instructions, medical literature or pathways. This leads to Problem Focused Knowledge Navigation that brings powerful efficiencies to the CMR. By recognizing the true workflow in the longitudinal diagnosis and management of any medical problem, the efficiency of the CMR is maximized. OHEAP allows for optimal use of both personal and external data elements in the medical record. Its powerful orientation attributes minimize the time spent in analyzing the current status of the problem while its connections to problem specific databases help resolve the problem.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Donnelly W. J., Brauner D. J. Why SOAP is bad for the medical record. Arch Intern Med. 1992 Mar;152(3):481–484. [PubMed] [Google Scholar]
- Forrey A. W., McDonald C. J., DeMoor G., Huff S. M., Leavelle D., Leland D., Fiers T., Charles L., Griffin B., Stalling F. Logical observation identifier names and codes (LOINC) database: a public use set of codes and names for electronic reporting of clinical laboratory test results. Clin Chem. 1996 Jan;42(1):81–90. [PubMed] [Google Scholar]
- Naeymi-Rad F. A feature dictionary supporting a multi-domain medical knowledge base. Comput Methods Programs Biomed. 1989 Oct-Nov;30(2-3):217–228. doi: 10.1016/0169-2607(89)90074-6. [DOI] [PubMed] [Google Scholar]
- Rubin A. S. Another way to enhance SOAP's usefulness. Acad Med. 1998 May;73(5):445–446. doi: 10.1097/00001888-199805000-00001. [DOI] [PubMed] [Google Scholar]
- Salmon P., Rappaport A., Bainbridge M., Hayes G., Williams J. Taking the problem oriented medical record forward. Proc AMIA Annu Fall Symp. 1996:463–467. [PMC free article] [PubMed] [Google Scholar]
- Warner H. R., Guo D., Mason C., Livingston J., Bray B. E. Enroute toward a computer based patient record: the ACIS project. Proc Annu Symp Comput Appl Med Care. 1995:152–156. [PMC free article] [PubMed] [Google Scholar]
- Weed L. L. Medical records that guide and teach. N Engl J Med. 1968 Mar 14;278(11):593–600. doi: 10.1056/NEJM196803142781105. [DOI] [PubMed] [Google Scholar]
- Weed L. L. New premises and new tools for medical care and education. J Dent Educ. 1996 Jan;60(1):64–67. [PubMed] [Google Scholar]