

Abstract
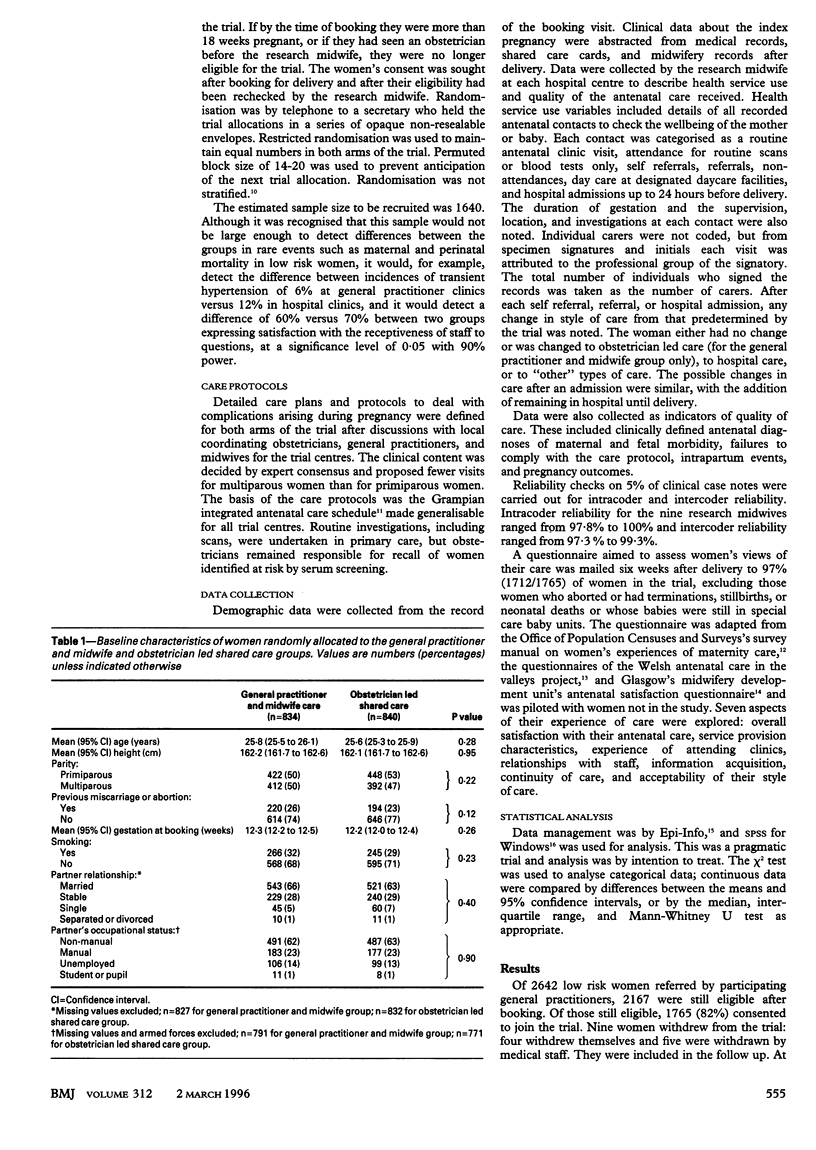
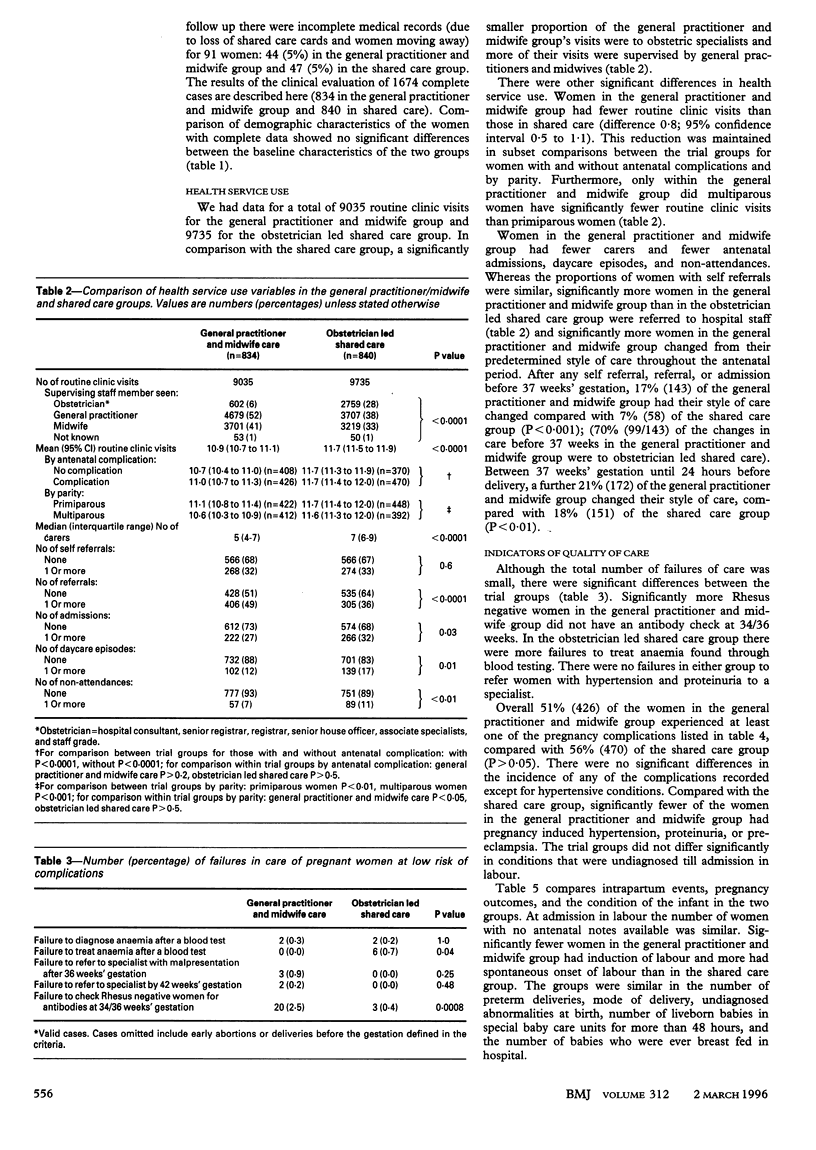
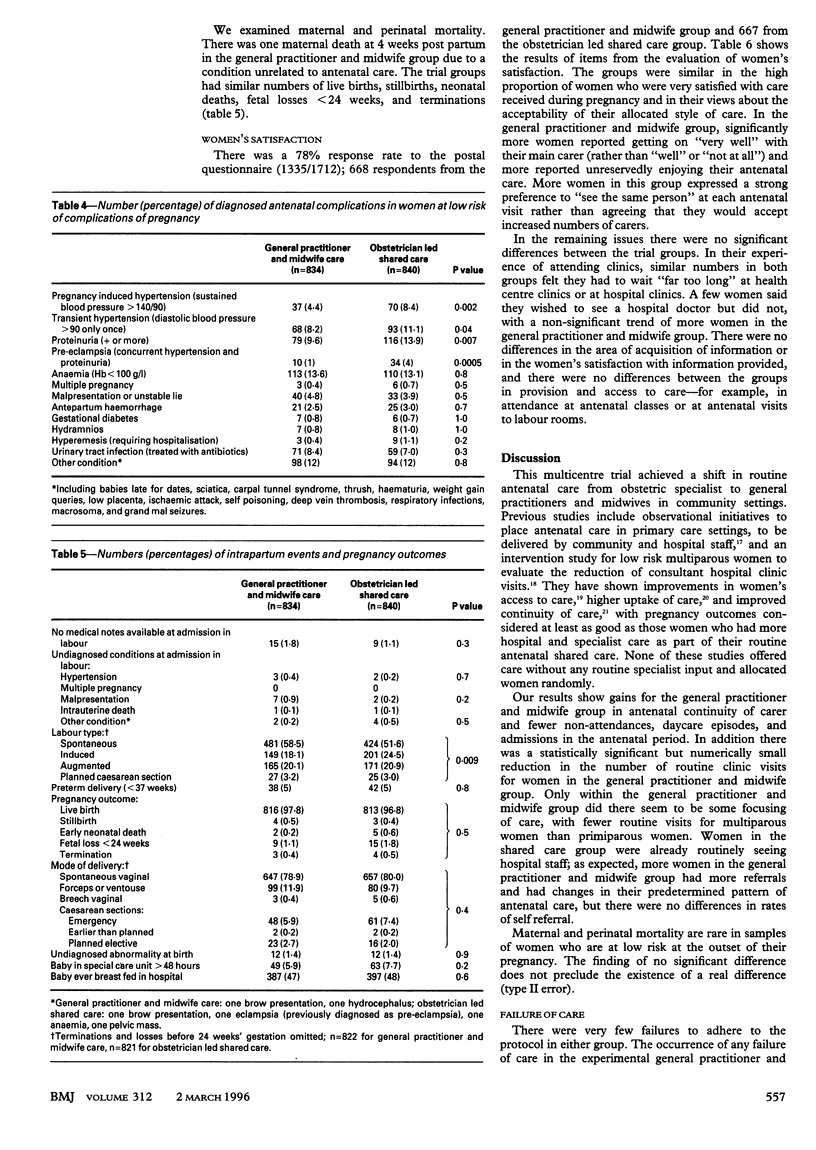
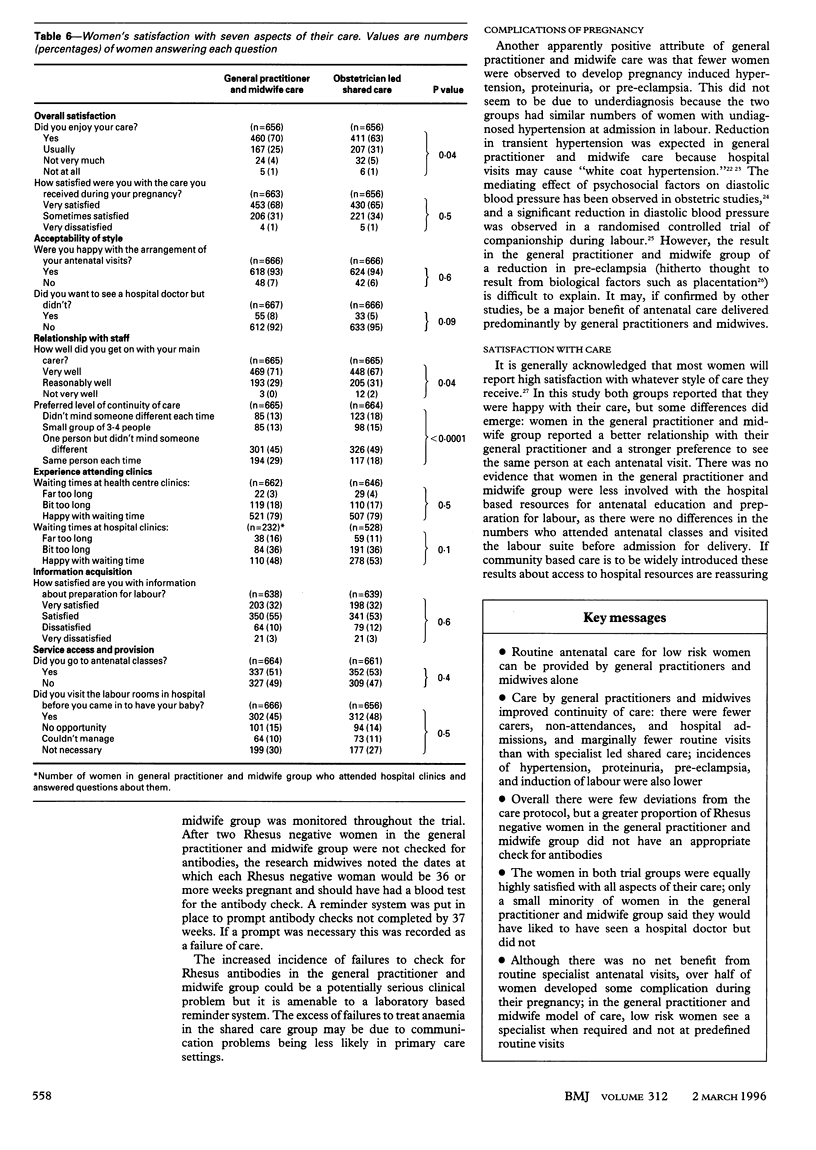
OBJECTIVE--To compare routine antenatal care provided by general practitioners and midwives with obstetrician led shared care. DESIGN--Multicentre randomised controlled trial. SETTING--51 general practices linked to nine Scottish maternity hospitals. SUBJECTS--1765 women at low risk of antenatal complications. INTERVENTION--Routine antenatal care by general practitioners and midwives according to a care plan and protocols for managing complications. MAIN OUTCOME MEASURES--Comparisons of health service use, indicators of quality of care, and women's satisfaction. RESULTS--Continuity of care was improved for the general practitioner and midwife group as the number of carers was less (median 5 carers v 7 for shared care group, P<0.0001) and the number of routine visits reduced (10.9 v 11.7, P<0.0001). Fewer women in the general practitioner and midwife group had antenatal admissions (27% (222/834) v 32% (266/840), P<0.05), non-attendances (7% (57) v 11% (89), P<0.01) and daycare (12% (102) v 7% (139), P<0.05) but more were referred (49% (406) v 36% (305), P<0.0001). Rates of antenatal diagnoses did not differ except that fewer women in the general practitioner and midwife group had hypertensive disorders (pregnancy induced hypertension, 5% (37) v 8% (70), P<0.01) and fewer had labour induced (18% (149) v 24% (201), P<0.01). Few failures to comply with the care protocol occurred, but more Rhesus negative women in the general practitioner and midwife group did not have an appropriate antibody check (2.5% (20) v 0.4% (3), P<0.0001). Both groups expressed high satisfaction with care (68% (453/663) v 65% (430/656), P=0.5) and acceptability of allocated style of care (93% (618) v 94% (624), P=0.6). Access to hospital support before labour was similar (45% (302) v 48% (312) visited labour rooms before giving birth, P=0.6). CONCLUSION--Routine specialist visits for women initially at low risk of pregnancy complications offer little or no clinical or consumer benefit.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Hall M. H., Chng P. K., MacGillivray I. Is routine antenatal care worth while? Lancet. 1980 Jul 12;2(8185):78–80. doi: 10.1016/s0140-6736(80)92950-5. [DOI] [PubMed] [Google Scholar]
- Hill A. M., Yudkin P. L., Bull D. J., Barlow D. H., Charnock F. M., Gillmer M. D. Evaluating a policy of reduced consultant antenatal clinic visits for low risk multiparous women. Qual Health Care. 1993 Sep;2(3):152–156. doi: 10.1136/qshc.2.3.152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofmeyr G. J., Nikodem V. C., Wolman W. L., Chalmers B. E., Kramer T. Companionship to modify the clinical birth environment: effects on progress and perceptions of labour, and breastfeeding. Br J Obstet Gynaecol. 1991 Aug;98(8):756–764. doi: 10.1111/j.1471-0528.1991.tb13479.x. [DOI] [PubMed] [Google Scholar]
- James D. K. Should obstetricians see women with normal pregnancies? Obstetricians should focus on problems. BMJ. 1995 Jan 7;310(6971):37–38. doi: 10.1136/bmj.310.6971.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Little B. C., Hayworth J., Benson P., Hall F., Beard R. W., Dewhurst J., Priest R. G. Treatment of hypertension in pregnancy by relaxation and biofeedback. Lancet. 1984 Apr 21;1(8382):865–867. doi: 10.1016/s0140-6736(84)91337-0. [DOI] [PubMed] [Google Scholar]
- Mancia G., Bertinieri G., Grassi G., Parati G., Pomidossi G., Ferrari A., Gregorini L., Zanchetti A. Effects of blood-pressure measurement by the doctor on patient's blood pressure and heart rate. Lancet. 1983 Sep 24;2(8352):695–698. doi: 10.1016/s0140-6736(83)92244-4. [DOI] [PubMed] [Google Scholar]
- Pickering T. G., James G. D., Boddie C., Harshfield G. A., Blank S., Laragh J. H. How common is white coat hypertension? JAMA. 1988 Jan 8;259(2):225–228. [PubMed] [Google Scholar]
- Porter M., Macintyre S. What is, must be best: a research note on conservative or deferential responses to antenatal care provision. Soc Sci Med. 1984;19(11):1197–1200. doi: 10.1016/0277-9536(84)90370-8. [DOI] [PubMed] [Google Scholar]
- Robson J., Boomla K., Savage W. Reducing delay in booking for antenatal care. J R Coll Gen Pract. 1986 Jun;36(287):274–275. [PMC free article] [PubMed] [Google Scholar]
- Thomas H., Draper J., Field S., Hare M. J. Evaluation of an integrated community antenatal clinic. J R Coll Gen Pract. 1987 Dec;37(305):544–547. [PMC free article] [PubMed] [Google Scholar]
- Tucker J., Florey C. D., Howie P., McIlwaine G., Hall M. Is antenatal care apportioned according to obstetric risk? The Scottish antenatal care study. J Public Health Med. 1994 Mar;16(1):60–70. doi: 10.1093/oxfordjournals.pubmed.a042937. [DOI] [PubMed] [Google Scholar]
- Wood J. A review of antenatal care initiatives in primary care settings. Br J Gen Pract. 1991 Jan;41(342):26–30. [PMC free article] [PubMed] [Google Scholar]