

Abstract
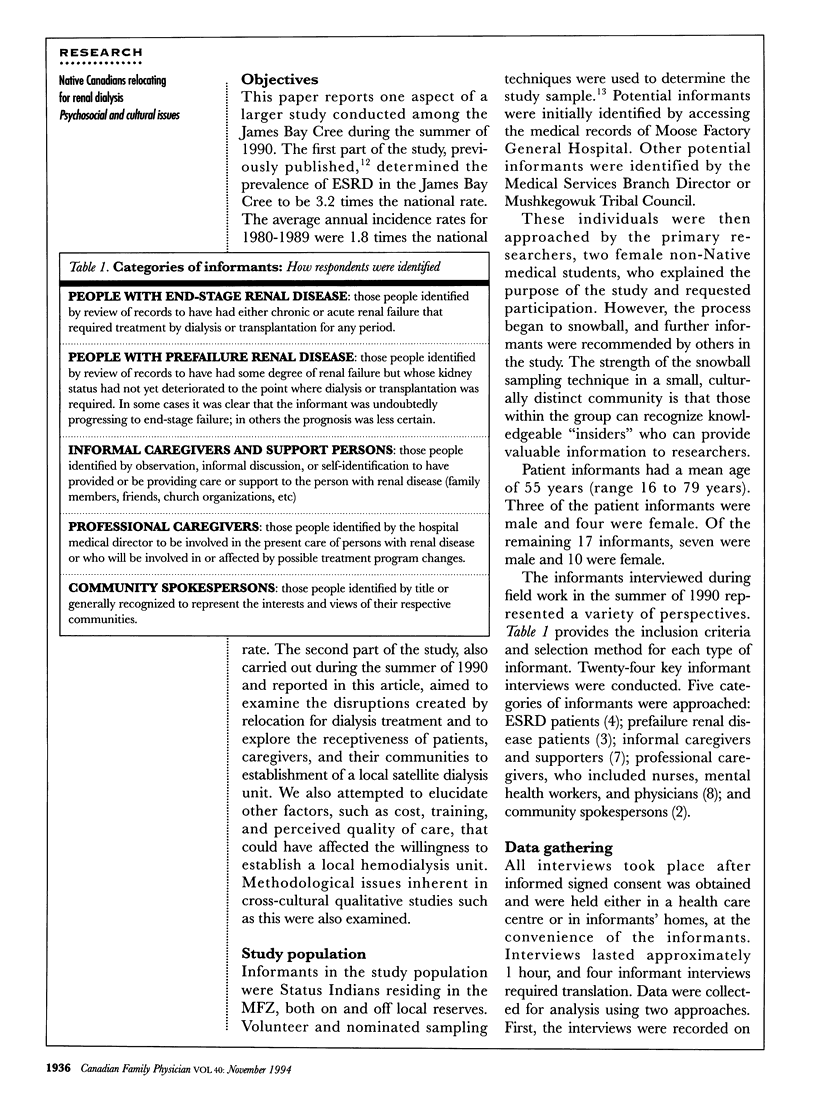
OBJECTIVE: To examine the effects of relocation from remote Native communities for dialysis treatment and explore the receptiveness of patients, caregivers, and their communities to establishing a local satellite dialysis unit. Second, to examine the methodological issues inherent in a qualitative, cross-cultural study. DESIGN: Qualitative descriptive survey using semistructured interviews. SETTING: The Moose Factory Zone (MFZ), situated along the west coast of James Bay in northern Ontario, is one of four geographically defined areas of responsibility within Ontario through which the federal government provides health care services to Native Canadians. PARTICIPANTS: Twenty-four Native residents of MFZ selected by volunteer and nominative sampling techniques. Patients with end-stage or prefailure renal disease, informal caregivers and supporters, professional caregivers, and community spokespersons were included in the study population. MAIN OUTCOME MEASURES: Identification of issues important in planning dialysis services for Native patients in remote communities in the MFZ. RESULTS: Informal caregivers and both categories of patients supported in principle a proposed satellite dialysis unit at Moose Factory General Hospital. Their criticisms of the present system necessitating relocation to urban centres included inadequate social support, inconvenience and expense, and family separation. Professional caregivers generally supported establishing a local dialysis unit but had concerns regarding staff training and continuity of care. Community spokespersons also supported the proposed unit but only if quality of care could be ensured. CONCLUSIONS: Relocation for dialysis treatment disrupts social support patterns and creates psychosocial problems. Although the psychosocial advantages of providing dialysis treatment services close to home are readily apparent, other considerations, such as cost, equipment, and expertise, and training of health care personnel, make the provision of tertiary level care more difficult in isolated areas. Additional study is required to determine the impact of methodological issues inherent in qualitative cross-cultural studies such as this.
Full text
PDF




Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bain H. W. Community development: an approach to health care of Indians. Can Med Assoc J. 1982 Feb 1;126(3):223–224. [PMC free article] [PubMed] [Google Scholar]
- Community-based health promotion surveys. Papers presented at the 78th annual conference of the Canadian Public Health Association. June 1987. Can J Public Health. 1988 Mar-Apr;79 (Suppl 1):1–31. [PubMed] [Google Scholar]
- Dyck R. F., Tan L. Rates and outcomes of diabetic end-stage renal disease among registered native people in Saskatchewan. CMAJ. 1994 Jan 15;150(2):203–208. [PMC free article] [PubMed] [Google Scholar]
- Farkas C. S., Shah C. Public health departments and Native health care in urban centres. Can J Public Health. 1986 Jul-Aug;77(4):274–277. [PubMed] [Google Scholar]
- Haffner S. M., Hazuda H. P., Mitchell B. D., Patterson J. K., Stern M. P. Increased incidence of type II diabetes mellitus in Mexican Americans. Diabetes Care. 1991 Feb;14(2):102–108. doi: 10.2337/diacare.14.2.102. [DOI] [PubMed] [Google Scholar]
- Kimmel P. L. Towards a developmental view of end-stage renal disease. Am J Kidney Dis. 1990 Mar;15(3):191–193. doi: 10.1016/s0272-6386(12)80761-x. [DOI] [PubMed] [Google Scholar]
- Krefting L. Rigor in qualitative research: the assessment of trustworthiness. Am J Occup Ther. 1991 Mar;45(3):214–222. doi: 10.5014/ajot.45.3.214. [DOI] [PubMed] [Google Scholar]
- Mardiros M. Primary health care and Canada's indigenous people. Can Nurse. 1987 Sep;83(8):20–24. [PubMed] [Google Scholar]
- Nuttall R. N. The development of Indian Boards of Health in Alberta. Can J Public Health. 1982 Sep-Oct;73(5):300–303. [PubMed] [Google Scholar]
- Reiss D. Patient, family, and staff responses to end-stage renal disease. Am J Kidney Dis. 1990 Mar;15(3):194–200. doi: 10.1016/s0272-6386(12)80762-1. [DOI] [PubMed] [Google Scholar]
- Rhoades E. R., Mason R. D., Eddy P., Smith E. M., Burns T. R. The Indian Health Service approach to alcoholism among American Indians and Alaska Natives. Public Health Rep. 1988 Nov-Dec;103(6):621–627. [PMC free article] [PubMed] [Google Scholar]
- Wilson R., Krefting L. H., Sutcliffe P., VanBussel L. Incidence and prevalence of end-stage renal disease among Ontario's James Bay Cree. Can J Public Health. 1992 Mar-Apr;83(2):143–146. [PubMed] [Google Scholar]
- Young T. K., McIntyre L. L., Dooley J., Rodriguez J. Epidemiologic features of diabetes mellitus among Indians in northwestern Ontario and northeastern Manitoba. Can Med Assoc J. 1985 Apr 1;132(7):793–797. [PMC free article] [PubMed] [Google Scholar]