

Abstract
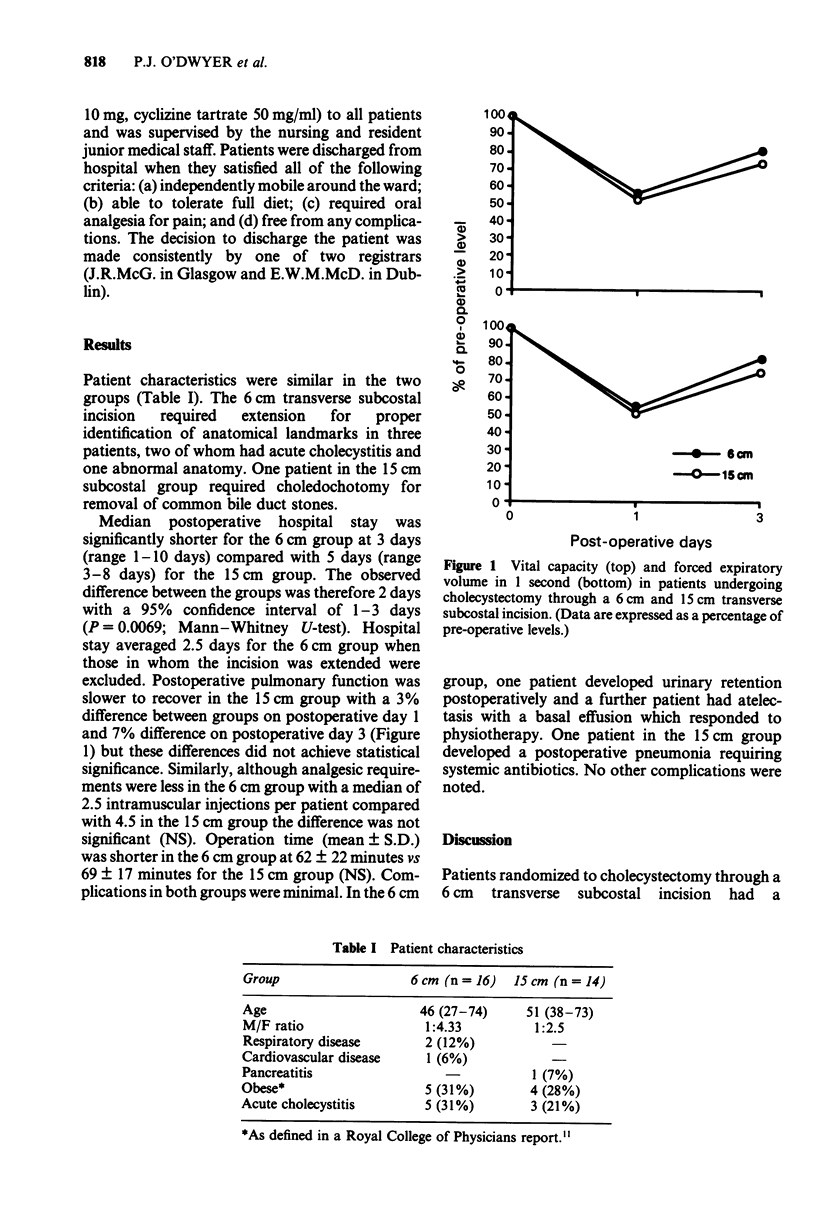
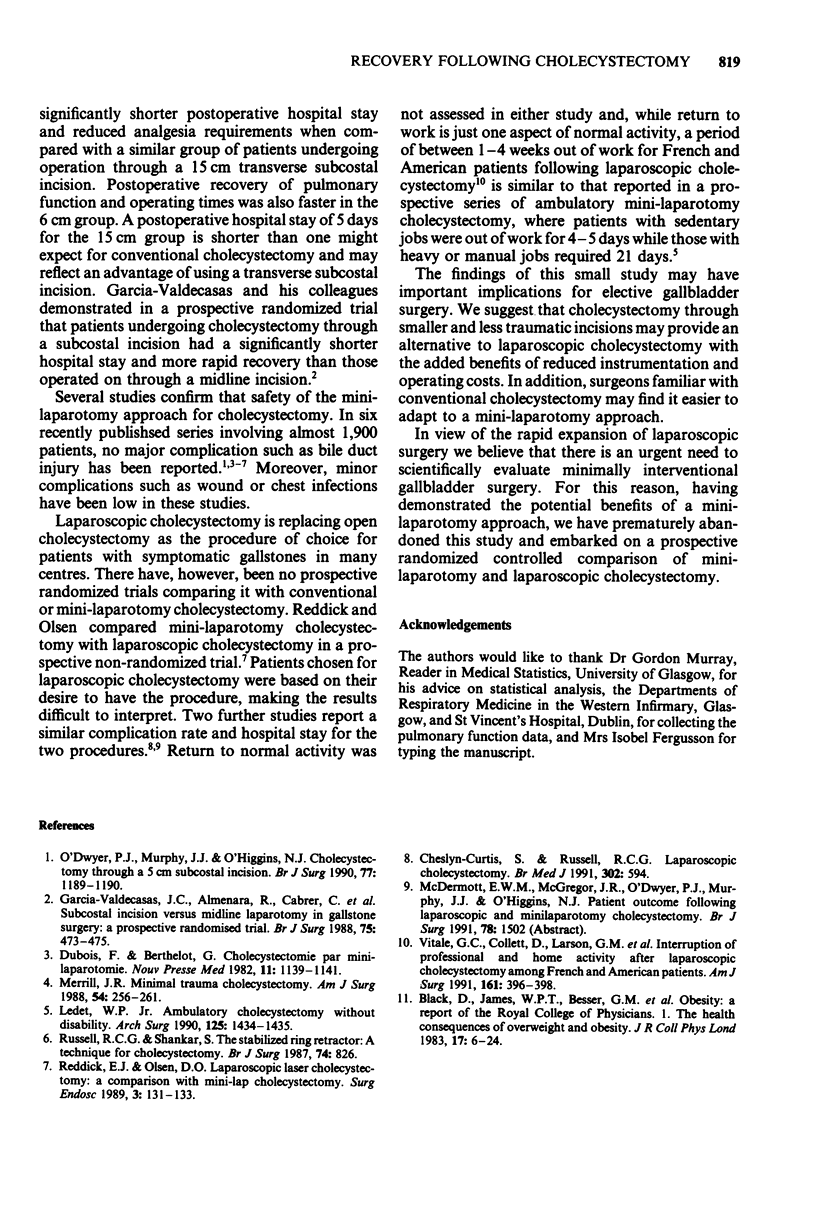
The effect of incision length on patient recovery following cholecystectomy has not been investigated previously. In this study, 30 patients with symptomatic gallstones were randomized to cholecystectomy through a 6 cm or 15 cm transverse subcostal incision. Postoperative hospital stay was significantly shorter in the 6 cm incision group (median 3 days vs 5 days; P = 0.0069 Mann-Whitney U-test). In the 6 cm group analgesic requirements were reduced (median 2.5 vs 4.5 intramuscular opiate injections per patient) and recovery of depressed postoperative pulmonary function (FVC and FEV1) was faster (3% difference between groups on day 1 and 7% on day 3), although these differences did not achieve statistical significance. These results suggest that the length of incision may influence patient recovery following elective cholecystectomy. This has important implications as surgery carried out through shorter and less traumatic incisions may offer a cost-effective alternative to laparoscopic cholecystectomy. Moreover, some surgeons may find mini-laparotomy cholecystectomy easier to adopt than laparoscopic techniques.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Dubois F., Berthelot B. Cholécystectomie par mini-laparotomie. Nouv Presse Med. 1982 Apr 3;11(15):1139–1141. [PubMed] [Google Scholar]
- García-Valdecasas J. C., Almenara R., Cabrer C., de Lacy A. M., Sust M., Taurá P., Fuster J., Grande L., Pera M., Sentis J. Subcostal incision versus midline laparotomy in gallstone surgery: a prospective and randomized trial. Br J Surg. 1988 May;75(5):473–475. doi: 10.1002/bjs.1800750523. [DOI] [PubMed] [Google Scholar]
- Ledet W. P., Jr Ambulatory cholecystectomy without disability. Arch Surg. 1990 Nov;125(11):1434–1435. doi: 10.1001/archsurg.1990.01410230028004. [DOI] [PubMed] [Google Scholar]
- Merrill J. R. Minimal trauma cholecystectomy (a "no-touch" procedure in a "well"). Am Surg. 1988 May;54(5):256–261. [PubMed] [Google Scholar]
- O'Dwyer P. J., Murphy J. J., O'Higgins N. J. Cholecystectomy through a 5 cm subcostal incision. Br J Surg. 1990 Oct;77(10):1189–1190. doi: 10.1002/bjs.1800771034. [DOI] [PubMed] [Google Scholar]
- Reddick E. J., Olsen D. O. Laparoscopic laser cholecystectomy. A comparison with mini-lap cholecystectomy. Surg Endosc. 1989;3(3):131–133. doi: 10.1007/BF00591357. [DOI] [PubMed] [Google Scholar]
- Russell R. C., Shankar S. The stabilized ring retractor: a technique for cholecystectomy. Br J Surg. 1987 Sep;74(9):826–826. doi: 10.1002/bjs.1800740925. [DOI] [PubMed] [Google Scholar]
- Vitale G. C., Collet D., Larson G. M., Cheadle W. G., Miller F. B., Perissat J. Interruption of professional and home activity after laparoscopic cholecystectomy among French and American patients. Am J Surg. 1991 Mar;161(3):396–398. doi: 10.1016/0002-9610(91)90606-e. [DOI] [PubMed] [Google Scholar]