

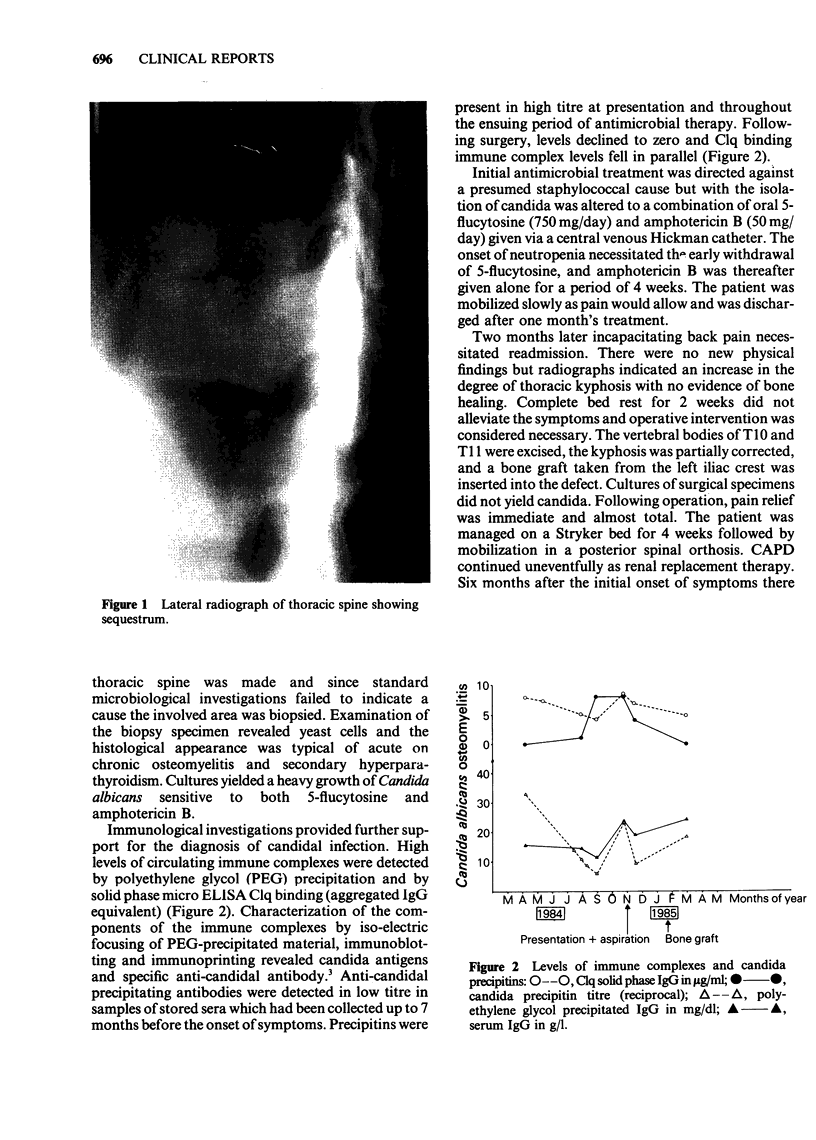
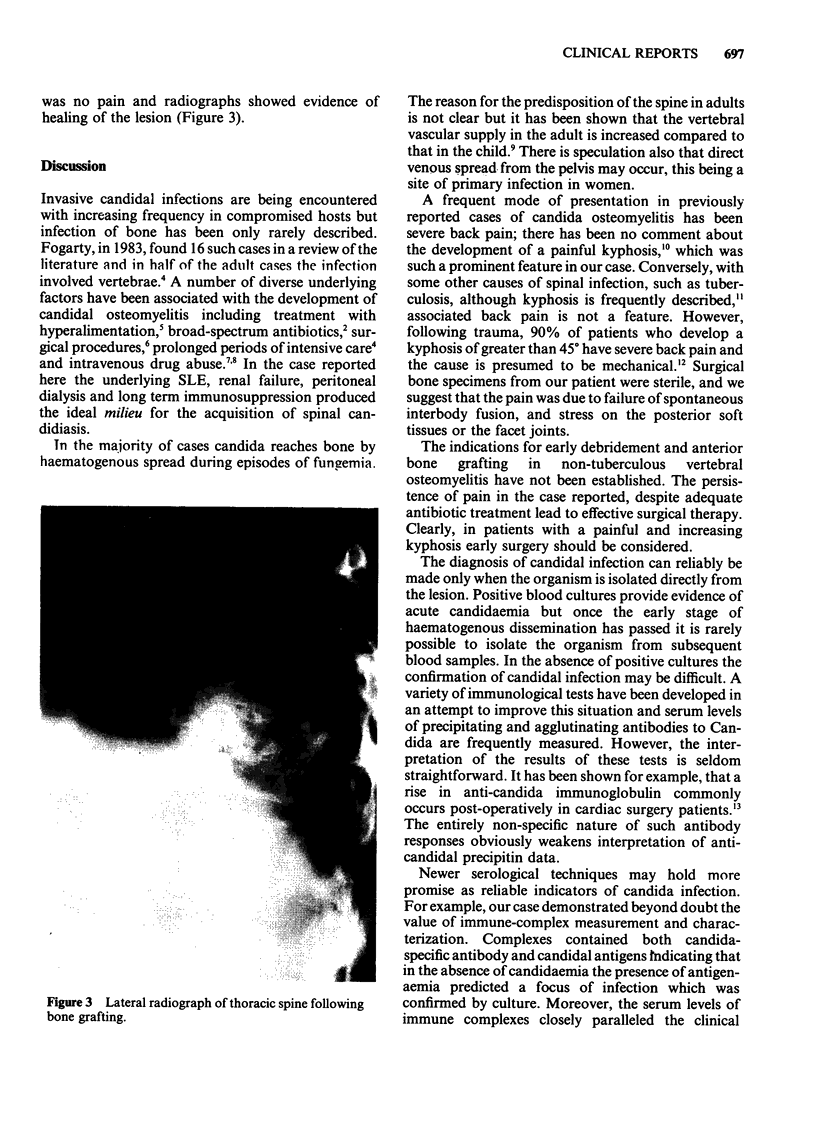
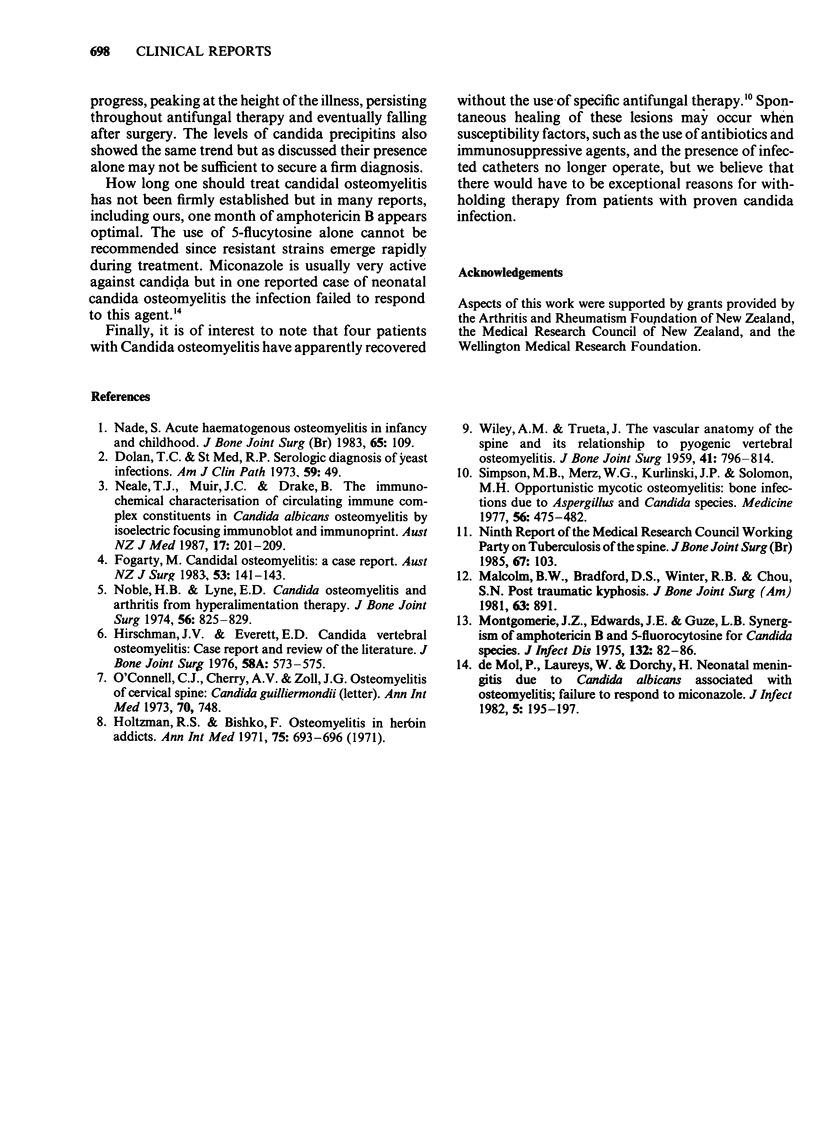
Abstract
Invasive candidal infections are encountered with increasing frequency in compromised hosts but bone infection is uncommon. A woman with systemic lupus erythematosus and end-stage renal failure managed by continuous ambulatory peritoneal dialysis developed a painful thoracic kyphosis and a lytic lesion in the vertebral bodies of T10 and T11. Blood cultures were sterile but bone biopsy material contained Candida albicans which also grew on culture. Circulating immune complexes were measured in high levels and contained candida antigens and specific anti-candida antibody as determined by isoelectric focusing, immunoblotting and immunoprinting techniques. Pain persisted after anti-fungal therapy had sterilized the lesion necessitating surgical excision of affected vertebrae, kyphosis correction and iliac crest bone grafting. The titres of circulating immune complexes and anti-candidal precipitins closely paralleled the clinical course.
Full text
PDF
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Fogarty M. Candidial osteomyelitis: a case report. Aust N Z J Surg. 1983 Apr;53(2):141–143. doi: 10.1111/j.1445-2197.1983.tb02415.x. [DOI] [PubMed] [Google Scholar]
- Holzman R. S., Bishko F. Osteomyelitis in heroin addicts. Ann Intern Med. 1971 Nov;75(5):693–696. doi: 10.7326/0003-4819-75-5-693. [DOI] [PubMed] [Google Scholar]
- Malcolm B. W., Bradford D. S., Winter R. B., Chou S. N. Post-traumatic kyphosis. A review of forty-eight surgically treated patients. J Bone Joint Surg Am. 1981 Jul;63(6):891–899. [PubMed] [Google Scholar]
- Montgomerie J. Z., Edwards J. E., Jr, Guze L. B. Synergism of amphotericin B and 5-fluorocytosine for candida species. J Infect Dis. 1975 Jul;132(1):82–86. doi: 10.1093/infdis/132.1.82. [DOI] [PubMed] [Google Scholar]
- Nade S. Acute haematogenous osteomyelitis in infancy and childhood. J Bone Joint Surg Br. 1983 Mar;65(2):109–119. doi: 10.1302/0301-620X.65B2.6826612. [DOI] [PubMed] [Google Scholar]
- Neale T. J., Muir J. C., Drake B. The immunochemical characterisation of circulating immune complex constituents in Candida albicans osteomyelitis by isoelectric focusing, immunoblot, and immunoprint. Aust N Z J Med. 1987 Apr;17(2):201–209. doi: 10.1111/j.1445-5994.1987.tb00041.x. [DOI] [PubMed] [Google Scholar]
- Noble H. B., Lyne E. D. Candida osteomyelitis and arthritis from hyperalimentation therapy. Case report. J Bone Joint Surg Am. 1974 Jun;56(4):825–829. [PubMed] [Google Scholar]
- O'Connell C. J., Cherry A. V., Zoll J. G. Letter: Osteomyelitis of cervical spine: candida guilliermondii. Ann Intern Med. 1973 Nov;79(5):748–748. doi: 10.7326/0003-4819-79-5-748_1. [DOI] [PubMed] [Google Scholar]
- Simpson M. B., Jr, Merz W. G., Kurlinski J. P., Solomon M. H. Opportunistic mycotic osteomyelitis: bone infections due to Aspergillus and Candida species. Medicine (Baltimore) 1977 Nov;56(6):475–482. [PubMed] [Google Scholar]
- WILEY A. M., TRUETA J. The vascular anatomy of the spine and its relationship to pyogenic vertebral osteomyelitis. J Bone Joint Surg Br. 1959 Nov;41-B:796–809. doi: 10.1302/0301-620X.41B4.796. [DOI] [PubMed] [Google Scholar]