

Abstract
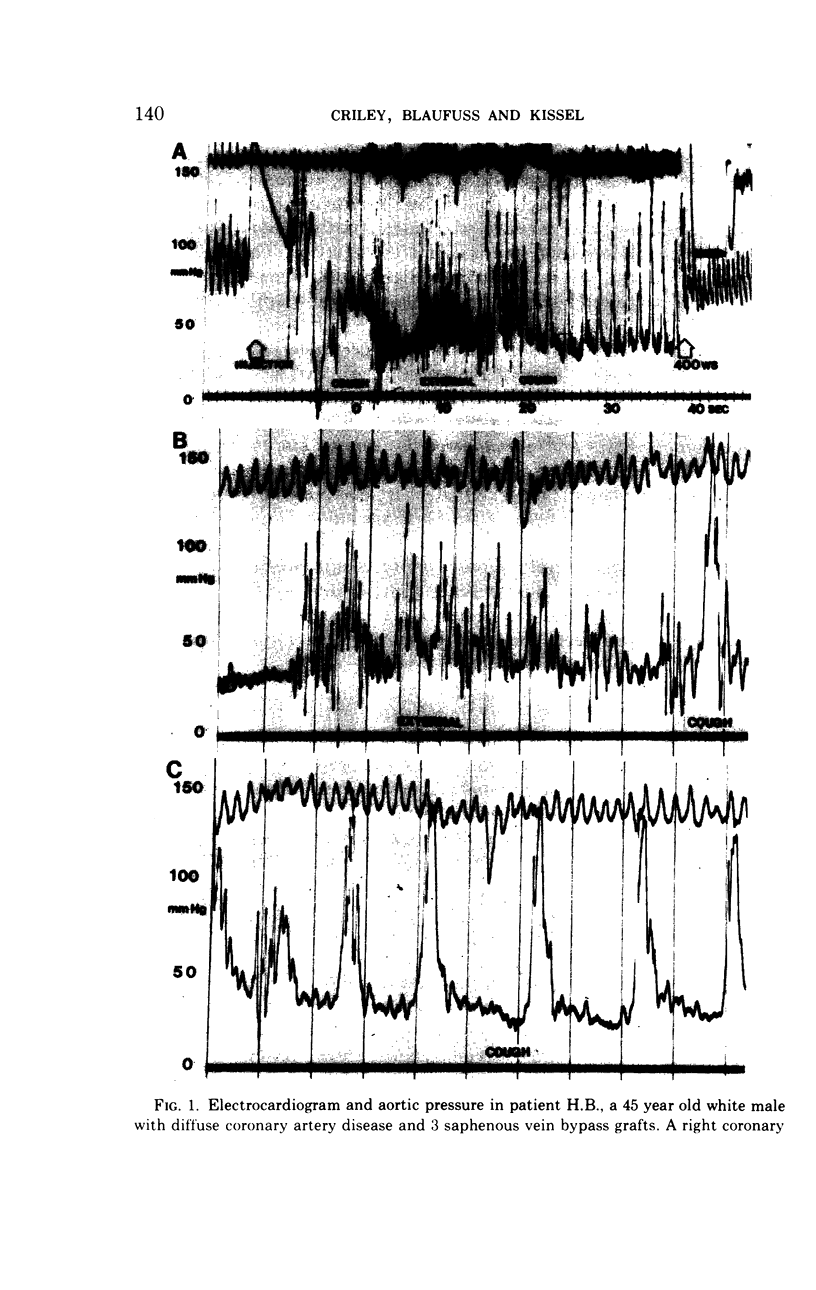
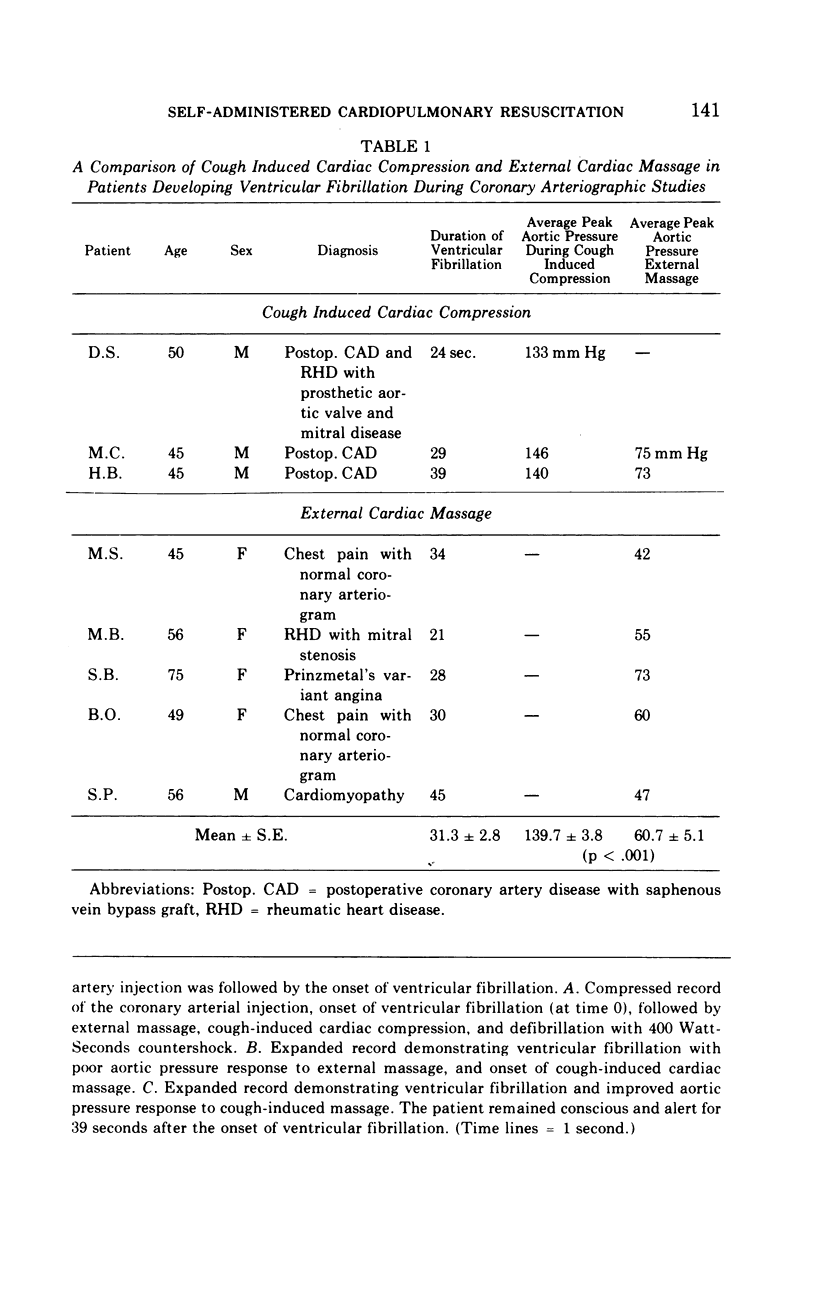
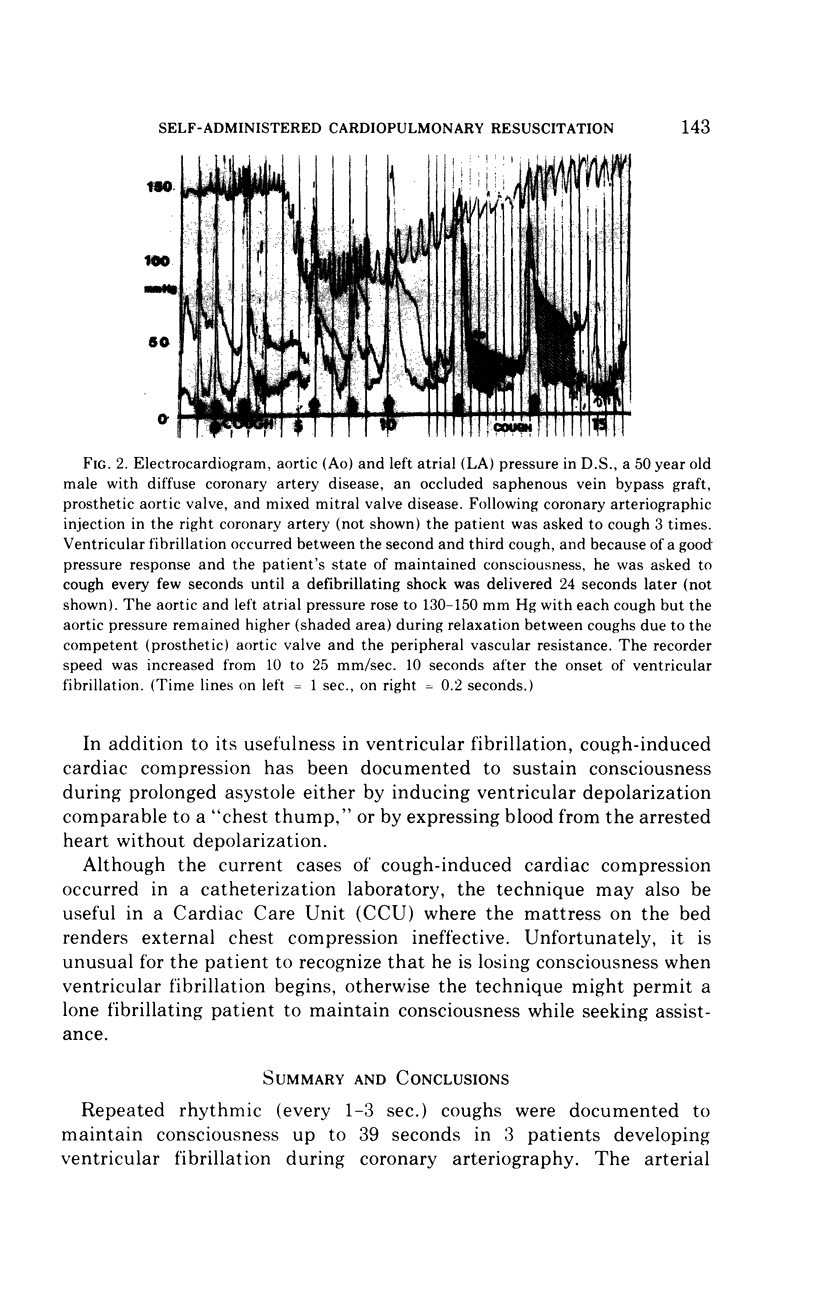
Repeated rhythmic (every 1-3 sec.) coughs were documented to maintain consciousness up to 39 seconds in 3 patients developing ventricular fibrillation during coronary arteriography. The arterial pressure wave resulting from a cough exceeded that induced by external chest compression in 2 individuals in whom both techniques were employed and in 5 others treated by external compression alone. Cough-induced cardiac compression is self-performed, and compared to external chest compression is less likely to traumatize the chest wall or heart and can be performed in any position on any surface. It is recommended that patients undergoing coronary arteriography be previously trained to cough abruptly and repeatedly every 1-3 seconds. The potential for utilizing this technique in other areas (i.e., CCU, home) is less favorable than in catheterization-induced ventricular fibrillation, but it might be employed successfully in patients with premonitory symptoms of ventricular arrhythmias or Stokes-Adams seizures. The prior training of high risk individuals (and their spouses) to induce effective coughing in the victim might be lifesaving.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Agdal N., Jorgensen T. G. Penetrating laceration of the pericardium and myocardium and myocardial rupture following closed-chest cardiac massage. Acta Med Scand. 1973 Nov;194(5):477–479. doi: 10.1111/j.0954-6820.1973.tb19474.x. [DOI] [PubMed] [Google Scholar]
- Burnside J., Daggett W. M., Austen W. G. Coronary artery rupture by a mitral valve prosthesis after closed chest massage. Ann Thorac Surg. 1970 Mar;9(3):267–271. doi: 10.1016/s0003-4975(10)65502-6. [DOI] [PubMed] [Google Scholar]
- CLARK D. T. Complications following closed-chest cardiac massage. JAMA. 1962 Jul 28;181:337–338. doi: 10.1001/jama.1962.03050300057020. [DOI] [PubMed] [Google Scholar]
- COHN L. H., SAYER W. J. Multiple complications from external cardiac massage. Report of a case. Calif Med. 1963 Apr;98:220–221. [PMC free article] [PubMed] [Google Scholar]
- Judkins M. P. Selective coronary arteriography. I. A percutaneous transfemoral technic. Radiology. 1967 Nov;89(5):815–824. doi: 10.1148/89.5.815. [DOI] [PubMed] [Google Scholar]
- KOUWENHOVEN W. B., JUDE J. R., KNICKERBOCKER G. G. Closed-chest cardiac massage. JAMA. 1960 Jul 9;173:1064–1067. doi: 10.1001/jama.1960.03020280004002. [DOI] [PubMed] [Google Scholar]
- MACKENZIE G. J., TAYLOR S. H., MCDONALD A. H., DONALD K. W. HAEMODYNAMIC EFFECTS OF EXTERNAL CARDIAC COMPRESSION. Lancet. 1964 Jun 20;1(7347):1342–1345. doi: 10.1016/s0140-6736(64)92036-7. [DOI] [PubMed] [Google Scholar]
- MORGAN R. R. Laceration of the liver from closed-chest cardiac massage. N Engl J Med. 1961 Jul 13;265:82–83. doi: 10.1056/NEJM196107132650207. [DOI] [PubMed] [Google Scholar]