

Abstract
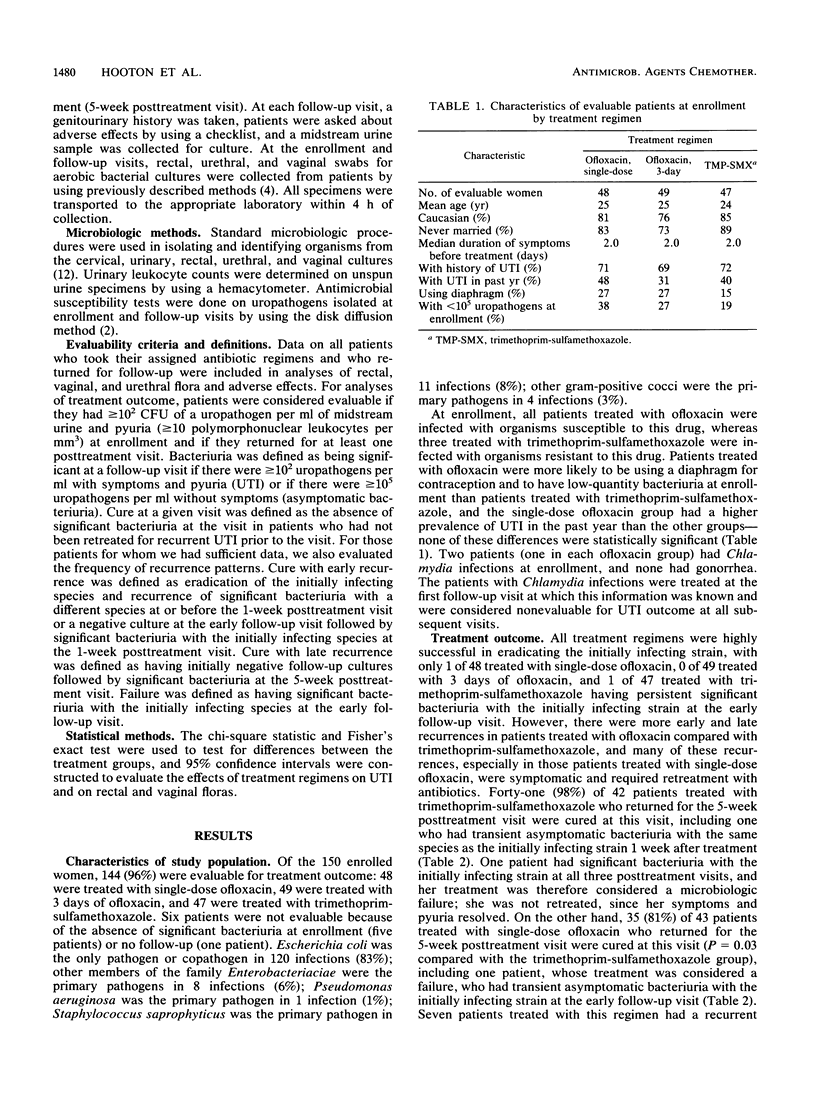
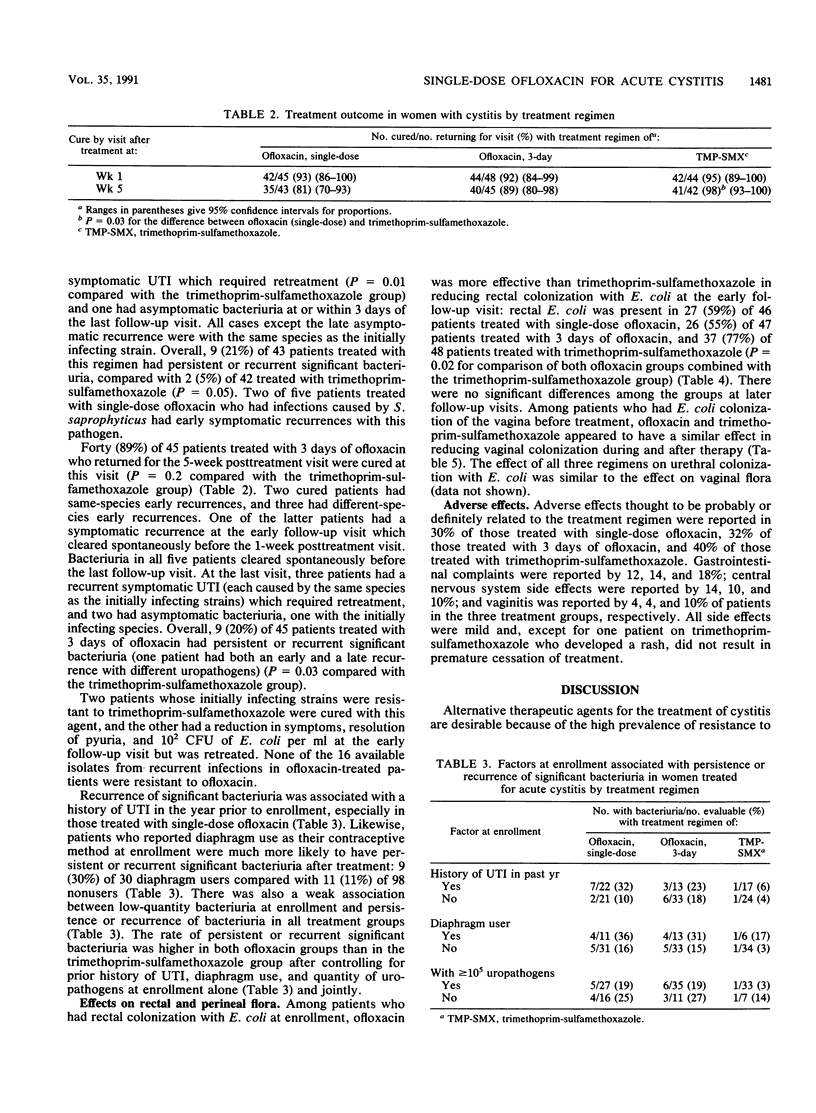
We compared the safety and efficacy of a single 400-mg dose of ofloxacin, ofloxacin (200 mg) once daily for 3 days, and trimethoprim-sulfamethoxazole (160:800 mg) twice daily for 7 days for the treatment of acute uncomplicated cystitis (urinary tract infection [UTI]) in women. At 5 weeks posttreatment, 35 (81%) of 43 patients treated with single-dose ofloxacin, 40 (89%) of 45 treated with 3 days of ofloxacin, and 41 (98%) of 42 treated with trimethoprim-sulfamethoxazole were cured (P = 0.03, single-dose ofloxacin group versus trimethoprim-sulfamethoxazole group). Retreatment for symptomatic recurrent UTI was given to 7 (16%) of 43 patients initially treated with single-dose ofloxacin, 3 (7%) of 45 patients treated with 3 days of ofloxacin, and 0 of 42 patients treated with trimethoprim-sulfamethoxazole (P = 0.01, single-dose ofloxacin group versus trimethoprim-sulfamethoxazole group). There was a trend in each of the three treatment groups toward an association between persistent or recurrent episodes of significant bacteriuria and a history of UTI in the past year and with diaphragm use. Ofloxacin was more effective than trimethoprim-sulfamethoxazole in eradicating Escherichia coli from rectal cultures during or soon after therapy, but there were no differences at later follow-up visits. Adverse effects were equally common among the three treatment groups. We conclude that single-dose ofloxacin was less effective than 7 days of trimethoprim-sulfamethoxazole for treatment of uncomplicated cystitis in women, while the 3-day ofloxacin regimen and the trimethoprim-sulfamethoxazole regimen were not significantly different in efficacy.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Arcieri G., Griffith E., Gruenwaldt G., Heyd A., O'Brien B., Becker N., August R. Ciprofloxacin: an update on clinical experience. Am J Med. 1987 Apr 27;82(4A):381–386. [PubMed] [Google Scholar]
- Bauer A. W., Kirby W. M., Sherris J. C., Turck M. Antibiotic susceptibility testing by a standardized single disk method. Am J Clin Pathol. 1966 Apr;45(4):493–496. [PubMed] [Google Scholar]
- Block J. M., Walstad R. A., Bjertnaes A., Hafstad P. E., Holte M., Ottemo I., Svarva P. L., Rolstad T., Peterson L. E. Ofloxacin versus trimethoprim-sulphamethoxazole in acute cystitis. Drugs. 1987;34 (Suppl 1):100–106. doi: 10.2165/00003495-198700341-00022. [DOI] [PubMed] [Google Scholar]
- Counts G. W., Stamm W. E., McKevitt M., Running K., Holmes K. K., Turck M. Treatment of cystitis in women with a single dose of trimethoprim-sulfamethoxazole. Rev Infect Dis. 1982 Mar-Apr;4(2):484–490. doi: 10.1093/clinids/4.2.484. [DOI] [PubMed] [Google Scholar]
- Fihn S. D., Johnson C., Roberts P. L., Running K., Stamm W. E. Trimethoprim-sulfamethoxazole for acute dysuria in women: a single-dose or 10-day course. A double-blind, randomized trial. Ann Intern Med. 1988 Mar;108(3):350–357. doi: 10.7326/0003-4819-108-3-350. [DOI] [PubMed] [Google Scholar]
- Ganguli L. A., Keaney M. G., Gould L. J. Norfloxacin: a three-day course for the treatment of urinary tract infection. Drugs Exp Clin Res. 1985;11(3):177–179. [PubMed] [Google Scholar]
- Garlando F., Rietiker S., Täuber M. G., Flepp M., Meier B., Lüthy R. Single-dose ciprofloxacin at 100 versus 250 mg for treatment of uncomplicated urinary tract infections in women. Antimicrob Agents Chemother. 1987 Feb;31(2):354–356. doi: 10.1128/aac.31.2.354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henry N. K., Schultz H. J., Grubbs N. C., Muller S. M., Ilstrup D. M., Wilson W. R. Comparison of ciprofloxacin and co-trimoxazole in the treatment of uncomplicated urinary tract infection in women. J Antimicrob Chemother. 1986 Nov;18 (Suppl 500):103–106. doi: 10.1093/jac/18.supplement_d.103. [DOI] [PubMed] [Google Scholar]
- Hooton T. M., Latham R. H., Wong E. S., Johnson C., Roberts P. L., Stamm W. E. Ofloxacin versus trimethoprim-sulfamethoxazole for treatment of acute cystitis. Antimicrob Agents Chemother. 1989 Aug;33(8):1308–1312. doi: 10.1128/aac.33.8.1308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson J. R., Stamm W. E. Urinary tract infections in women: diagnosis and treatment. Ann Intern Med. 1989 Dec 1;111(11):906–917. doi: 10.7326/0003-4819-111-11-906. [DOI] [PubMed] [Google Scholar]
- Leigh D. A., Walsh B., Harris K., Hancock P., Travers G. Pharmacokinetics of ofloxacin and the effect on the faecal flora of healthy volunteers. J Antimicrob Chemother. 1988 Sep;22 (Suppl 100):115–125. doi: 10.1093/jac/22.supplement_c.115. [DOI] [PubMed] [Google Scholar]
- Ludwig G., Pauthner H. Clinical experience with ofloxacin in upper and lower urinary tract infections. A comparison with co-trimoxazole and nitrofurantoin. Drugs. 1987;34 (Suppl 1):95–99. doi: 10.2165/00003495-198700341-00021. [DOI] [PubMed] [Google Scholar]
- Murray B. E., Rensimer E. R., DuPont H. L. Emergence of high-level trimethoprim resistance in fecal Escherichia coli during oral administration of trimethoprim or trimethoprim--sulfamethoxazole. N Engl J Med. 1982 Jan 21;306(3):130–135. doi: 10.1056/NEJM198201213060302. [DOI] [PubMed] [Google Scholar]
- Norrby S. R. Short-term treatment of uncomplicated lower urinary tract infections in women. Rev Infect Dis. 1990 May-Jun;12(3):458–467. doi: 10.1093/clinids/12.3.458. [DOI] [PubMed] [Google Scholar]
- Ode B., Walder M., Forsgren A. Failure of a single dose of 100 mg ofloxacin in lower urinary tract infections in females. Scand J Infect Dis. 1987;19(6):677–679. doi: 10.3109/00365548709117203. [DOI] [PubMed] [Google Scholar]
- Peddie B. A., Bailey R. R., Wells J. E. Resistance of urinary tract isolates of Escherichia coli to cotrimoxazole, sulphonamide, trimethoprim and ampicillin: an 11-year survey. N Z Med J. 1987 Jun 10;100(825):341–342. [PubMed] [Google Scholar]
- Rao D. S., Parfitt A. M., Villanueva A. R., Dorman P. J., Kleerekoper M. Hypophosphatemic osteomalacia and adult Fanconi syndrome due to light-chain nephropathy. Another form of oncogenous osteomalacia. Am J Med. 1987 Feb;82(2):333–338. doi: 10.1016/0002-9343(87)90081-7. [DOI] [PubMed] [Google Scholar]
- Raz R., Genesin J., Gonen E., Shmilovitz M., Hefter H., Potasman I. Single low-dose ofloxacin for the treatment of uncomplicated urinary tract infection in young women. J Antimicrob Chemother. 1988 Dec;22(6):945–949. doi: 10.1093/jac/22.6.945. [DOI] [PubMed] [Google Scholar]
- Raz R., Rottensterich E., Hefter H., Kennes Y., Potasman I. Single-dose ciprofloxacin in the treatment of uncomplicated urinary tract infection in women. Eur J Clin Microbiol Infect Dis. 1989 Dec;8(12):1040–1042. doi: 10.1007/BF01975166. [DOI] [PubMed] [Google Scholar]
- Schaeffer A. J., Sisney G. A. Efficacy of norfloxacin in urinary tract infection biological effects on vaginal and fecal flora. J Urol. 1985 Apr;133(4):628–630. doi: 10.1016/s0022-5347(17)49118-x. [DOI] [PubMed] [Google Scholar]
- Vellucci A., Bernardini G., Battaglia A. M., Battaglia P. Ofloxacin vs. cotrimoxazole in patients with complicated urinary tract infections. Int J Clin Pharmacol Ther Toxicol. 1987 May;25(5):279–281. [PubMed] [Google Scholar]
- Wolfson J. S., Hooper D. C. Treatment of genitourinary tract infections with fluoroquinolones: activity in vitro, pharmacokinetics, and clinical efficacy in urinary tract infections and prostatitis. Antimicrob Agents Chemother. 1989 Oct;33(10):1655–1661. doi: 10.1128/aac.33.10.1655. [DOI] [PMC free article] [PubMed] [Google Scholar]