

Abstract
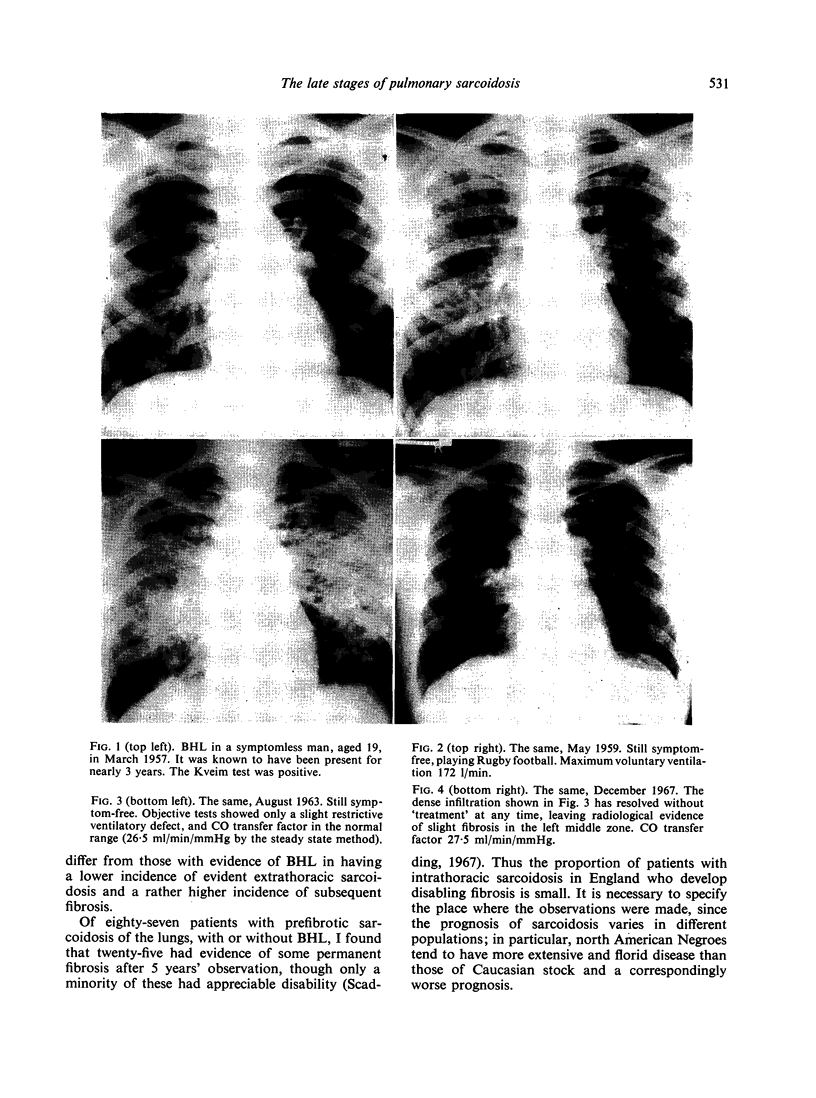
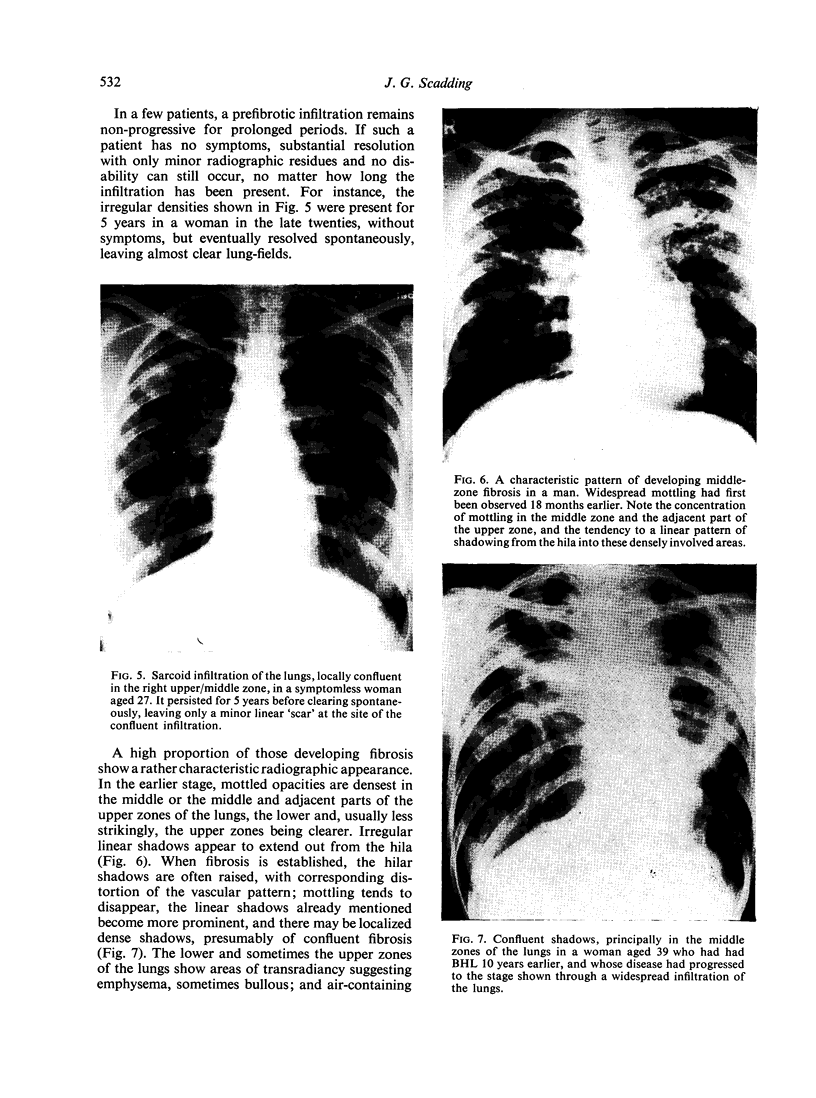
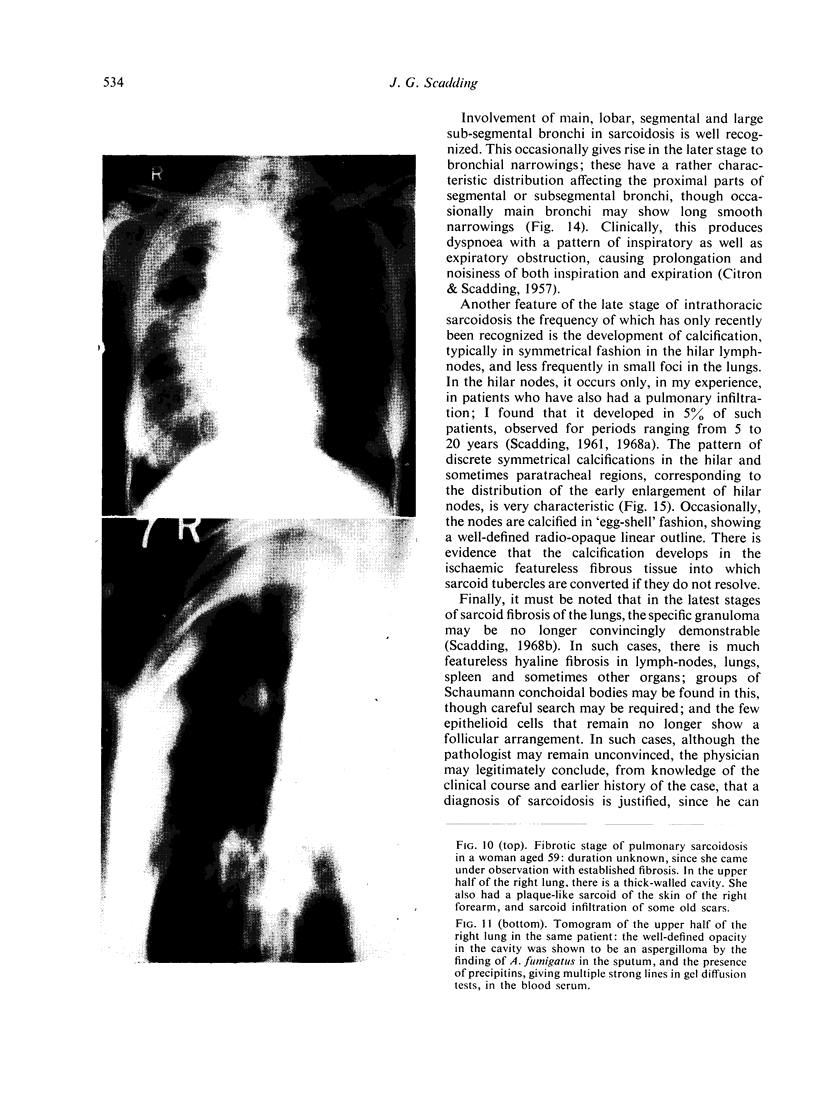
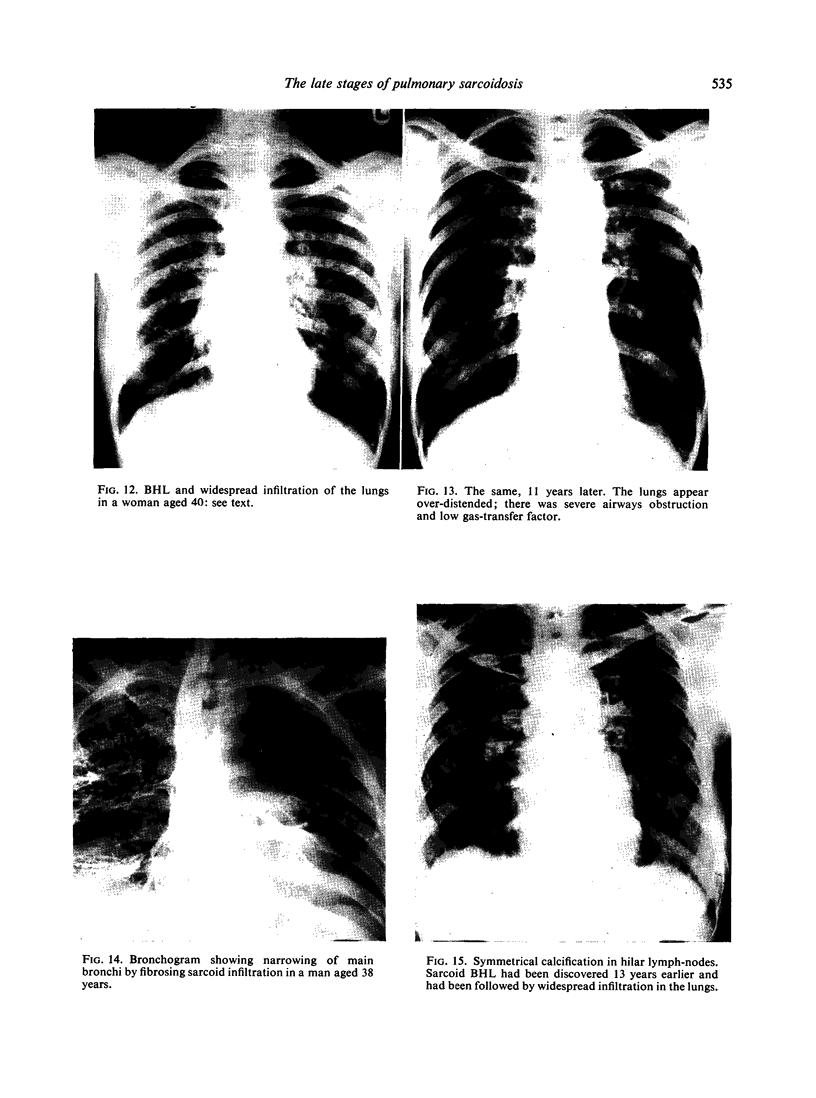
Pulmonary sarcoidosis is frequently preceded by bilateral hilar lymph-node enlargement (BHL). Although it is normally difficult to be certain in a patient without BHL that a stage of BHL has not in fact occurred in the past but been missed, there is good evidence that some cases of pulmonary sarcoidosis arise without preceding BHL. Although a prefibrotic infiltration of the lungs will usually show signs either of resolution or of developing fibrosis within 2 years, such an infiltration may remain apparently non-progressive, producing little functional defect, for much longer than this, and in such a case, substantial resolution remains possible. A high proportion of those who develop fibrosis show a characteristic pattern of strand-like fibrosis in the middle zones and lower part of the upper zones of the lungs, with emphysematous changes above and below. In densely fibrotic parts of the lungs, cavities may appear, probably from necrosis at the centres of large masses of hyaline fibrosis. A rare complication is the development of a ‘fungus ball’ due to the growth of Aspergillus in such a cavity.
Occasionally, fine focal fibrosis develops without distortion of lung architecture, but with severe disability.
A rare but important event is the development of bronchial stenoses. These may affect main, segmental or subsegmental bronchi, more especially the proximal parts of segmental or subsegmental bronchi.
Calcification has been observed to develop in a characteristic symmetrical fashion in the hilar lymphnodes and occasionally in small foci in the lungs in about 5% of patients with pulmonary sarcoidosis who initially had BHL, followed for periods ranging from 5 to 20 years.
In the late stages of sarcoid fibrosis of the lungs, the specific granuloma may be no longer convincingly demonstrable.
Full text
PDF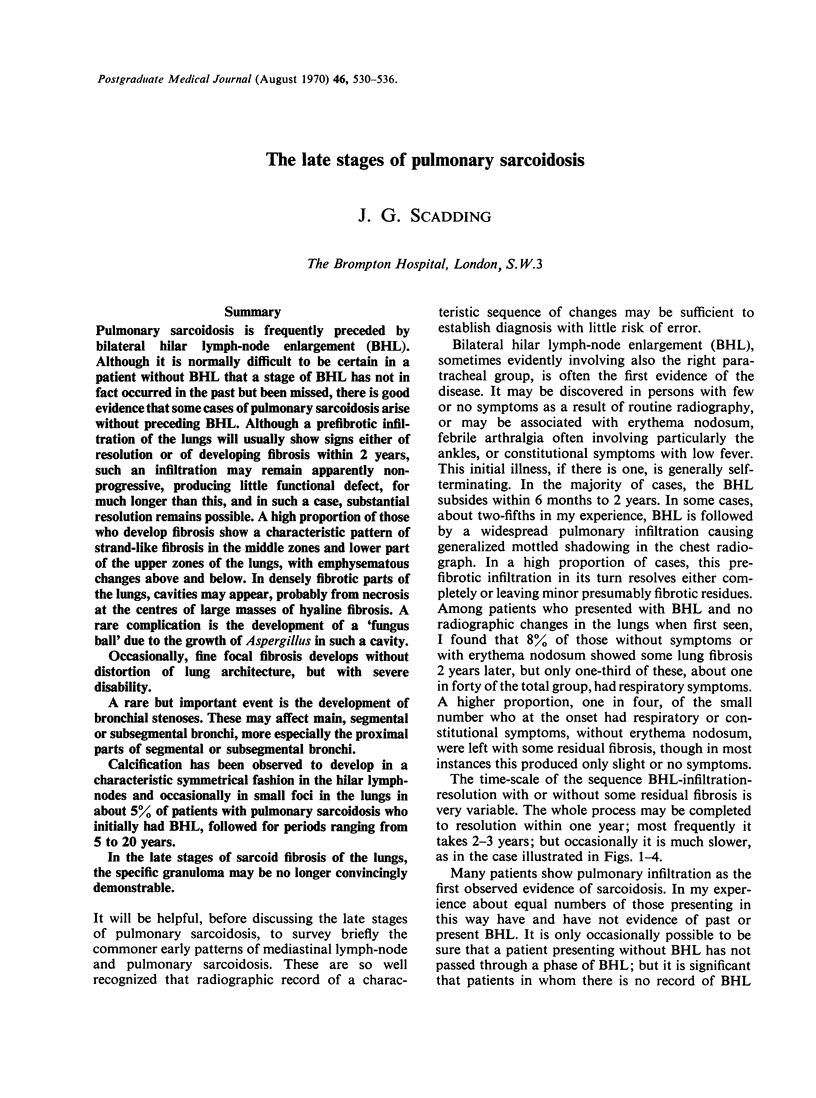
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- CITRON K. M., SCADDING J. G. Stenosing non-caseating tuberculosis (sarcoidosis) of the bronchi. Thorax. 1957 Mar;12(1):10–17. doi: 10.1136/thx.12.1.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SCADDING J. G. Calcification in sarcoidosis. Tubercle. 1961 Jun;42:121–135. doi: 10.1016/s0041-3879(61)80088-3. [DOI] [PubMed] [Google Scholar]
- Scadding J. G. A 'burnt-out' case of sarcoidosis. Postgrad Med J. 1968 Jan;44(507):105–108. doi: 10.1136/pgmj.44.507.105. [DOI] [PMC free article] [PubMed] [Google Scholar]