

Abstract
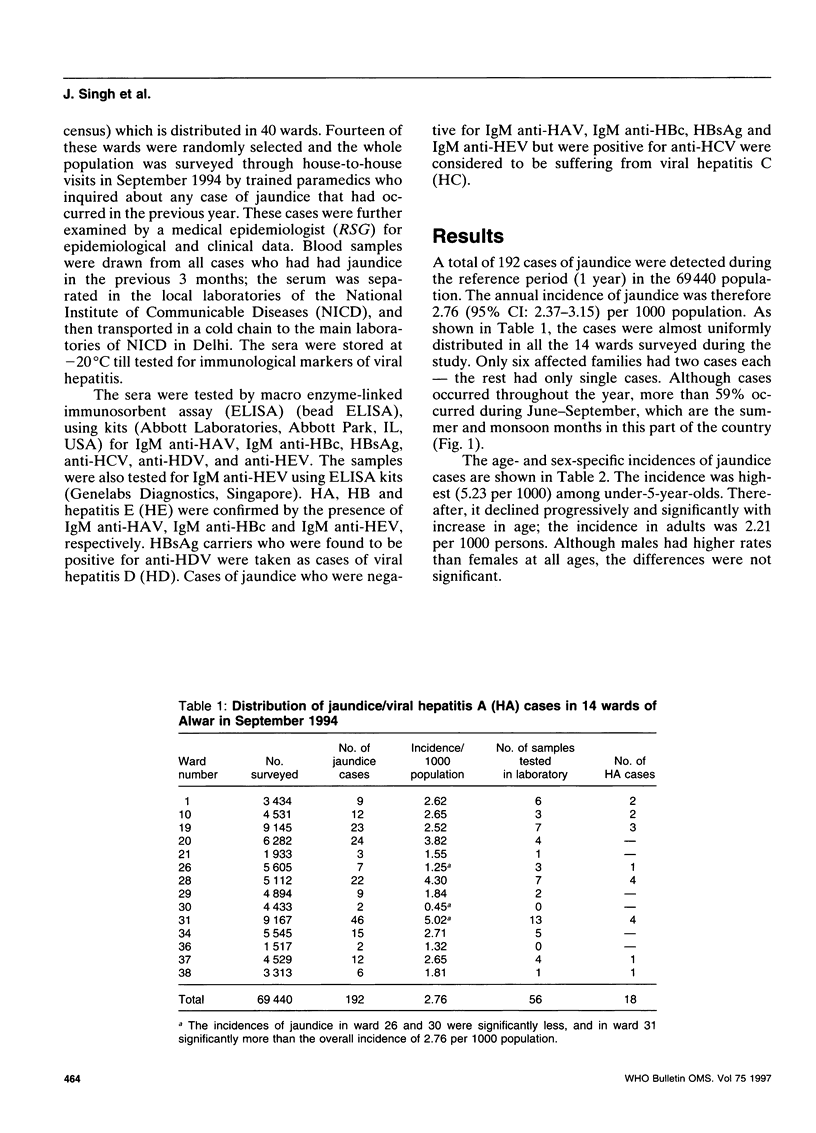
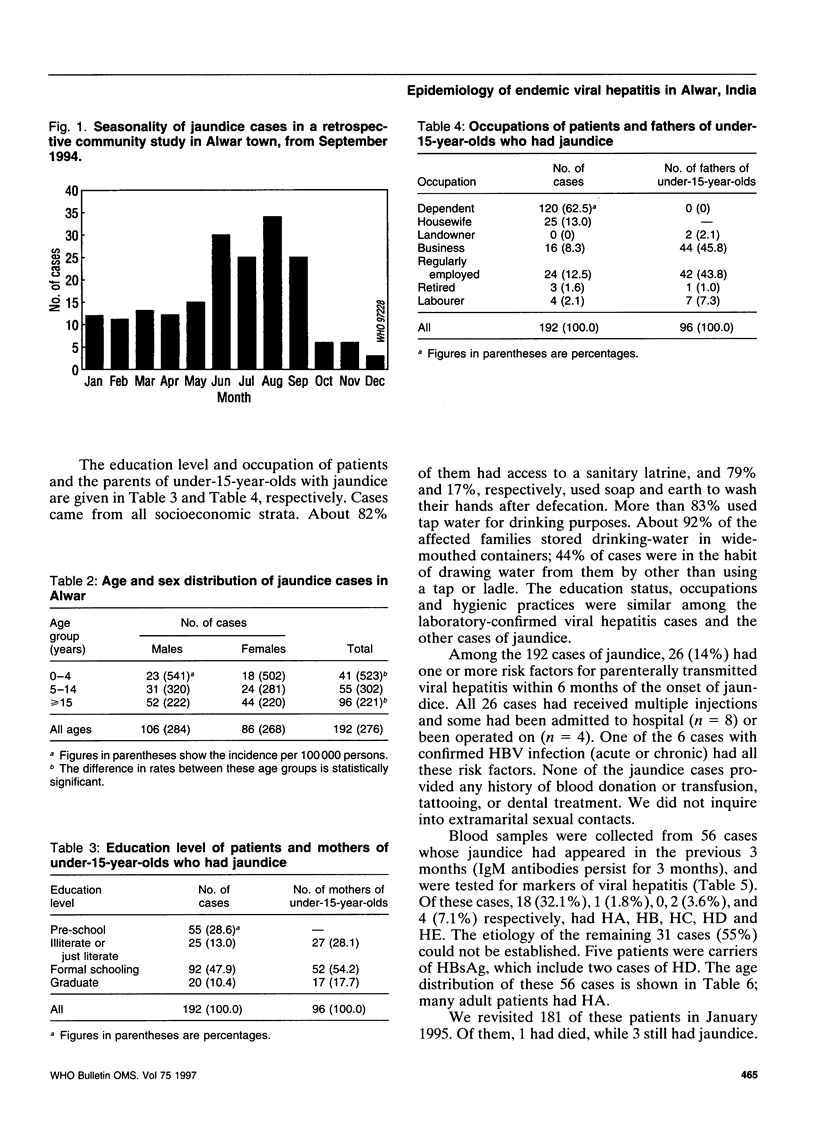
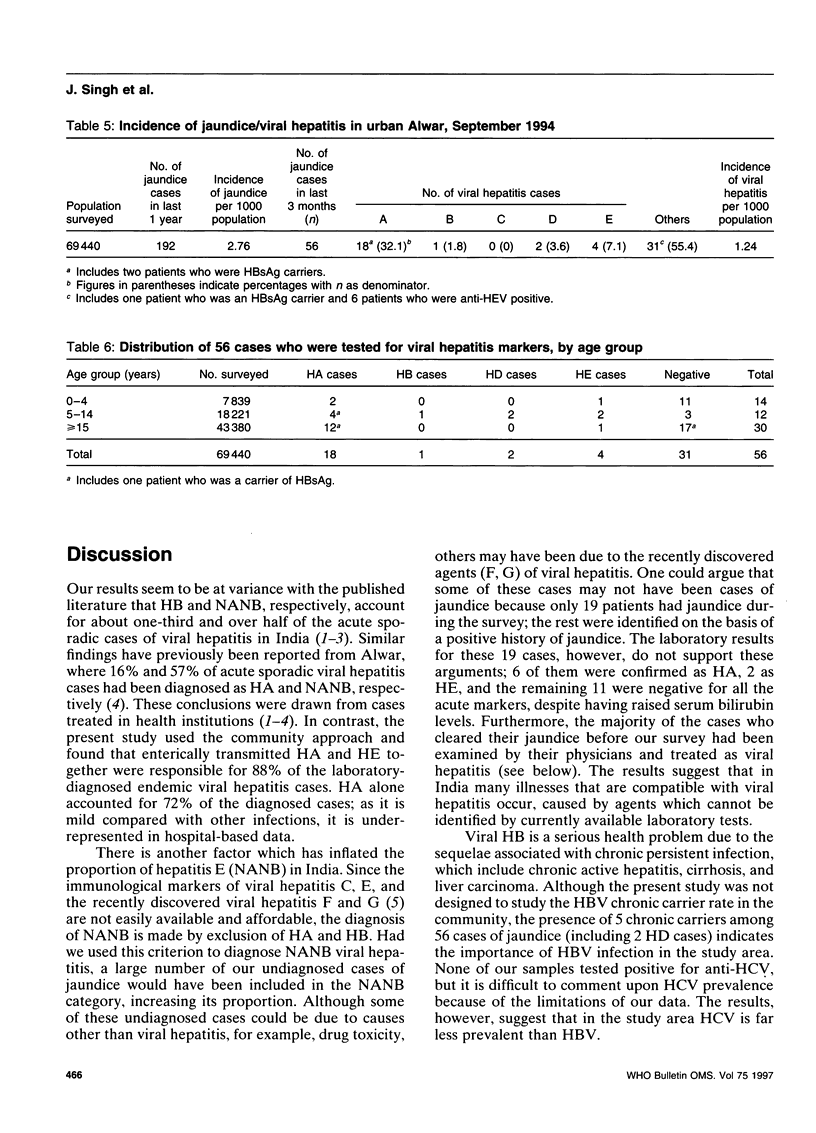
In a community study during a reference period of 1 year, 192 cases of jaundice were detected in an urban population of 69,440 in Alwar, Rajasthan. Detected by paramedics and confirmed by physicians, these cases gave an annual incidence of 2.76 (95% CI: 2.37-3.15) per 1000 population. At least one of these patients died, giving a case fatality ratio of 0.6%. The jaundice cases occurred in all areas investigated, and affected all socioeconomic strata. About 94% of the affected families had only single cases. Although cases occurred throughout the year, more than 59% occurred during June-September, which are the summer and monsoon months. The incidence was highest (5.23 per 1000) among under-5-year-olds and declined progressively and significantly thereafter. Males had a higher incidence than females at all ages; the differences were not significant. Blood samples from 56 cases who had jaundice in the last 3 months of the reference period were tested for markers of viral hepatitis. Of these, 18 (32.1%), 1 (1.8%), 0, 2 (3.6%), and 4 (7.1%) were found to have hepatitis A, B, C, D and E, respectively. The etiology of the remaining 31 cases (55%) could not be established; previously, they would have been included in the NANB (non-A, non-B) category, inflating its proportion. Hepatitis A (HA) was the predominant type; being comparatively mild, it is perhaps underrepresented in hospital-based data. Many HA cases were in adults, which may be the beginning of an age shift of HA to the right owing to improvements in living standards of the study population. Five cases were carriers of hepatitis B virus (HBV), indicating the importance of HBV infection in India as well. Finally, the study found the annual incidence of laboratory-supported cases of viral hepatitis to be 1.24 (95% CI: 0.98-1.5) per 1000 population, which suggests that it is a major public health problem in India.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bowden D. S., Moaven L. D., Locarnini S. A. New hepatitis viruses: are there enough letters in the alphabet? Med J Aust. 1996 Jan 15;164(2):87–89. doi: 10.5694/j.1326-5377.1996.tb101355.x. [DOI] [PubMed] [Google Scholar]
- Jain D. C., Singh J., Sebastian M., Sharma R. S. Viral hepatitis in Alwar during 1986-1988. J Commun Dis. 1992 Dec;24(4):247–248. [PubMed] [Google Scholar]
- Khuroo M. S., Duermeyer W., Zargar S. A., Ahanger M. A., Shah M. A. Acute sporadic non-A, non-B hepatitis in India. Am J Epidemiol. 1983 Sep;118(3):360–364. doi: 10.1093/oxfordjournals.aje.a113643. [DOI] [PubMed] [Google Scholar]
- Poovorawan Y., Theamboonlers A., Chumdermpadetsuk S. Changing seroepidemiology of hepatitis A virus infection in Thailand. Southeast Asian J Trop Med Public Health. 1993 Jun;24(2):250–254. [PubMed] [Google Scholar]
- Tandon B. N., Gandhi B. M., Joshi Y. K., Irshad M., Gupta H. Hepatitis virus non-A, non-B: the cause of a major public health problem in India. Bull World Health Organ. 1985;63(5):931–934. [PMC free article] [PubMed] [Google Scholar]