

Abstract
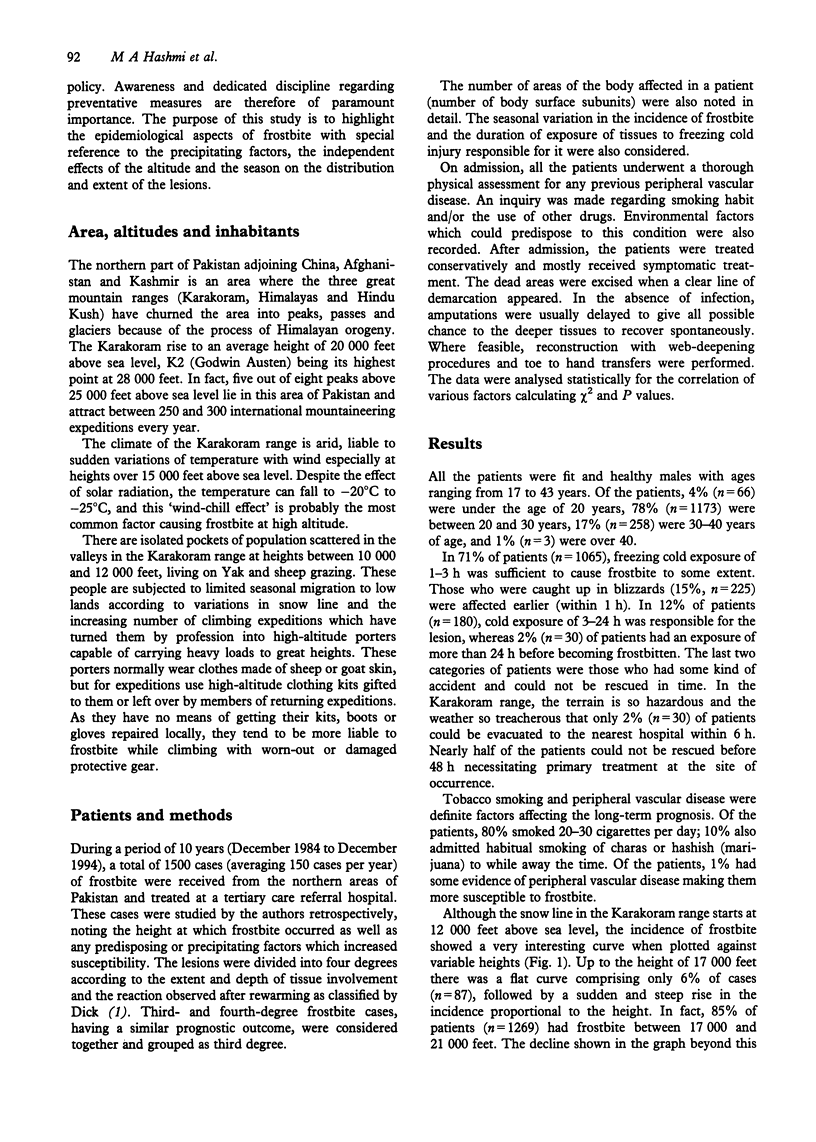
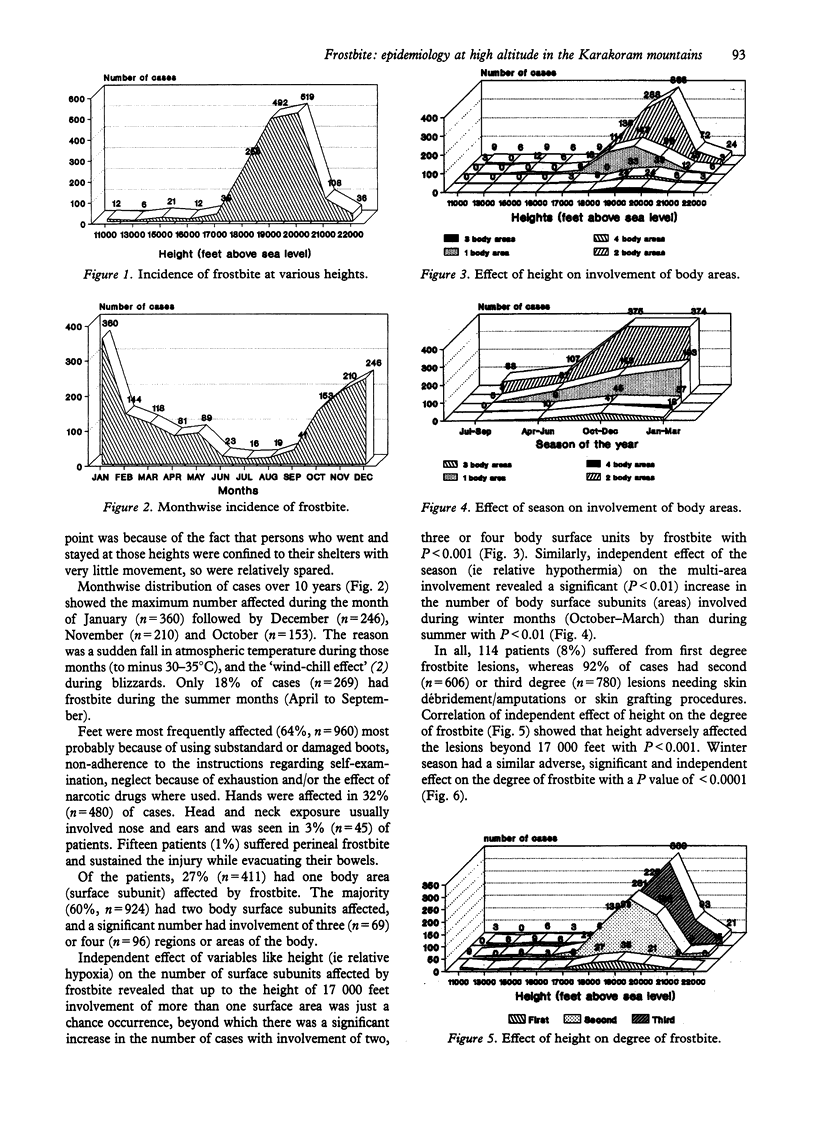
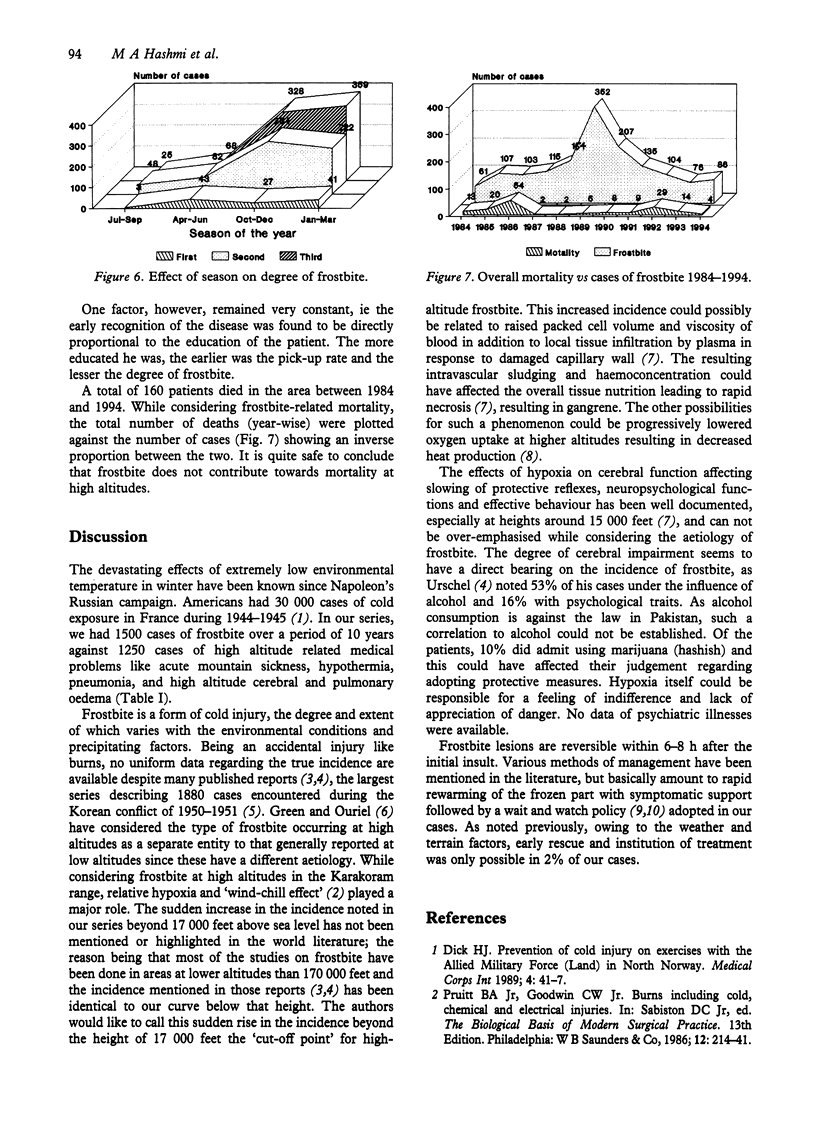
During a 10-year period (December 1984 to December 1994), 1500 cases of frostbite were treated at a tertiary care medical facility. They were all males with their ages ranging from 17 to 43 years. All the patients sustained the frostbite injury in the northeastern part of Pakistan known as the Karakoram range of mountains. They included a large number of porters and guides employed by various mountaineering expeditions (approximately 250-300 expeditions per year) in that region, as well as local inhabitants. This retrospective study included the heights at which frostbite occurred (range 11,000-22,000 feet above sea level). Of the patients, 15% (n = 225) got frostbitten within 1 h of exposure, whereas the majority (71%) had an exposure of 1-3 h. The effect of seasonal variations (relative hypothermia) on the extent and depth (degree) of frostbite and the distribution of lesions as per body surface subunits (areas) was noted and found to be statistically significant with P < 0.05 for both. The occurrence of frostbite at various heights showed a very steep upward curve beyond a height of 17,000 feet above sea level. This has been termed the 'cut-off' point for frostbite by the authors, the increase depicting the true picture of 'high altitude frostbite'. Tobacco smoking and peripheral vascular disease were found to be important contributing factors. The feet were involved most frequently (64%) followed by the hands (32%), the head and neck region (3%) and the perineum (1%). Independent effects of the height (relative hypoxia) on the depth of frostbite lesion (degree) and on the involvement of multiple body areas (surface subunits) showed significant correlation with P values well below 0.05 for each. Of cases, 92% (n = 1386) had second- or third-degree frostbite necessitating definitive surgical intervention. Total frostbite-related mortality spanned over 10 years was 11%.
Full text
PDF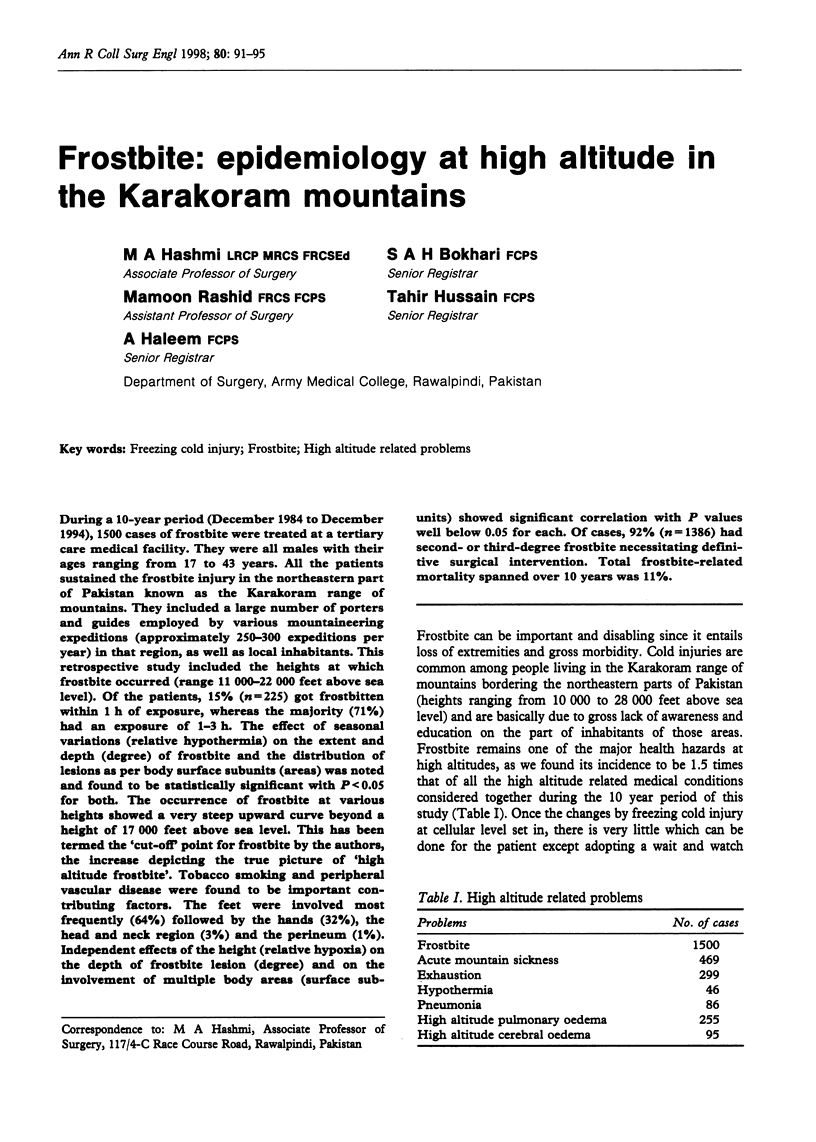
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Britt L. D., Dascombe W. H., Rodriguez A. New horizons in management of hypothermia and frostbite injury. Surg Clin North Am. 1991 Apr;71(2):345–370. doi: 10.1016/s0039-6109(16)45384-3. [DOI] [PubMed] [Google Scholar]
- Taylor M. S. Cold weather injuries during peacetime military training. Mil Med. 1992 Nov;157(11):602–604. [PubMed] [Google Scholar]
- Urschel J. D. Frostbite: predisposing factors and predictors of poor outcome. J Trauma. 1990 Mar;30(3):340–342. doi: 10.1097/00005373-199003000-00015. [DOI] [PubMed] [Google Scholar]
- Vogel J. E., Dellon A. L. Frostbite injuries of the hand. Clin Plast Surg. 1989 Jul;16(3):565–576. [PubMed] [Google Scholar]